
Abstract
Ellagic acid (EA) is a polyphenolic compound with antiviral activity against chikungunya, a rapidly spreading new tropical disease transmitted to humans by mosquitoes and now affecting millions worldwide. The most common symptoms of chikungunya virus infection are fever and joint pain. Other manifestations of infection can include encephalitis and an arthritic joint swelling with pain that may persist for months or years after the initial infection. The disease has recently spread to the U.S.A., with locally-transmitted cases of chikungunya virus reported in Florida. There is no approved vaccine to prevent or medicine to treat chikungunya virus infections. In this study, the Estimated Daily Intake (EDI) of EA from the food supply established using the National Health and Nutrition Examination Survey (NHANES) is used to set a maximum dose of an EA formulation for a high priority clinical trial.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
1.1 Compound
Ellagic acid (EA) is a polyphenolic compound with health benefits including antioxidant, anti-inflammatory, anti-proliferative, athero-protective, anti-hepatotoxic and anti-viral properties [1, 2]. EA is found in many plant extracts, fruits and nuts, usually in the form of hydrolyzable ellagitannins that are complex esters of EA with glucose. Natural sources high in ellagitannins include a variety of plant extracts including green tea, nuts such as walnuts, pecans and almonds, and fruits, particularly berries, such as blackberries, raspberries and strawberries, as well as grapes and pomegranates.
1.2 Chikungunya
Chikungunya virus is transmitted to humans by mosquitoes. Typical symptoms of chikungunya virus infection are fever and joint pain. Other manifestations may include headache, encephalitis, muscle pain, rash, and an arthritis-like joint swelling with pain that may persist for months or years after the initial infection. The word ‘chikungunya’ is thought to be derived from its description in the Makonde language, meaning “that which bends up” the deformed posture of people with the severe joint pain and arthritic symptoms associated with this disease (Chikungunya-Wikipedia, https://en.wikipedia.org/wiki/Chikungunya). There is no vaccine to prevent or medicine to treat chikungunya virus infections.
Millions of people worldwide suffer from chikungunya infections. The disease spreads quickly once it is established in an area. Outbreaks of chikungunya have occurred in countries in Africa, Asia, Europe, and the Indian and Pacific Oceans. Before 2006, chikungunya virus disease was only rarely pinpointed in U.S. travelers. In 2006–2013, studies found a mean of 28 people per year in the United States with positive tests for recent chikungunya infection. All of these people were travelers visiting or returning to the United States from affected areas in Asia, Africa, or the Indian Ocean.
In late 2013, the first local transmission of chikungunya virus in the Americas was identified on the island of St. Martin, and since then all of the other Caribbean countries and territories. (Local transmission means that mosquitoes in the area have been infected with the virus and are spreading it to people.)
Beginning in 2014, chikungunya virus disease cases were reported among U.S. travelers returning from affected areas in the Americas and local transmission was identified in Florida, Puerto Rico, and the U.S. Virgin Islands. In 2014, there were 11 locally-transmitted cases of chikungunya virus in the U.S. All were reported in Florida. There were 2,781 travel-associated cases reported in the U.S. The first locally acquired cases of chikungunya were reported in Florida on July 17, 2014. These cases represent the first time that mosquitoes in the continental United States are thought to have spread the virus to non-travelers. Unfortunately, this new disease seems certain to spread quickly. Data Driven Computational Science (DDCS) offers ways to accelerate drug development in response to the spread of this disease.
EA has been shown to be an inhibitor of chikungunya virus replication in high throughput screening of small molecules for chikungunya [3]. In screening a natural products library of 502 compounds from Enzo Life Sciences, EA at 10 µM produced 99.6% inhibition of chikungunya in an in vitro assay.
1.3 Metabolism
Ellagitannins are broken down in the intestine to eventually release EA. The bioavailability of ellagitannins and EA have been shown to be low in both humans and in animal models, likely because the compounds are hydrophobic and they because are metabolized by gut microorganisms [4,5,6,7]. The amount of ellagitannins and EA reaching the systemic circulation and peripheral tissues after ingestion is small to none [6]. It is established that ellagitannins are not absorbed while there is high variability in EA and EA metabolites found in human plasma after ingestion of standardized amounts of ellagitannins and EA [8,9,10]. These studies indicate that small amounts of EA are absorbed and detectable in plasma with a Cmax of approximately 100 nM (using standardized doses) and a Tmax of 1 h [8, 9]. EA is metabolized to glucuronides and methyl-glucuronide derivatives in the plasma. The most common metabolite found in urine and plasma is EA dimethyl ether glucuronide [11].
It appears that the majority of ingested ellagitannins and EA are metabolized by the gut microbiota into a variety of urolithins. Urolithins are dibenzopyran-6-one derivatives that are produced from EA through the loss of one of the two lactones present in EA and then by successive removal of hydroxyl groups. Urolithin D is produced first, followed sequentially by urolithin C, urolithin A, and urolithin B. Urolithins appear in the circulatory system almost exclusively as glucuronide, sulfate and methylated forms as a result of phase II metabolism after absorption in the colon and passage through the liver [12]. While the amount of EA in the circulation is in the nanomolar range, urolithins and their glucuronide and sulfate conjugates circulate at concentrations in the range of 0.2–20 μM [13]. In light of the much larger concentrations of urolithins in the circulation compared to EA, it is must be considered that the reported in vivo health effects of ellagitannin and EA may be largely due to the gut-produced urolithins. Growing evidence, mostly in vitro, supports the idea that urolithins have many of the same effects as EA in vitro. Various studies have shown evidence of anti-inflammatory [14,15,16], anticarcinogenic [17,18,19,20], anti-glycative [21], possibly antioxidant [5, 22], and antimicrobial [23] effects of urolithins.
There is variation in how people metabolize EA into the various urolithins [24,25,26]. This is not surprising in light of the known differences between individuals in intestinal microbiotic composition. Tomás-Barberán [25] evaluated the urinary urolithin profiles of healthy volunteers after consuming walnuts and pomegranate extracts. They found that, consistent with previous findings, that urolithin A was the main metabolite produced in humans. However, they noted that the subjects could be divided into three groups based on their urinary profiles of urolithins. One group excreted only urolithin A metabolites while a second group excreted urolithin A and isourolithin A in addition to urolithin B. The third group had undetectable levels of urolithins in their urine. These results suggest that people will benefit differently from eating ellagitannin rich foods.
1.4 Use of EDI
Knowledge of the Estimated Daily Intake (EDI) can permit pharmacokinetic and formulation studies to be conducted without prior expensive and time-consuming toxicology studies, especially when the molecule is naturally present in the food supply (see Fig. 1). A subject’s dietary level of the compound would normally vary around the EDI. A subject is brought in to the drug evaluation unit, and after the usual ICH E6 procedures and informed consent, is “washed out” of any of the compound might be present from previous food consumption. Typically, washout is accomplished by maintaining the subject on a diet containing none of the compound to be investigated for a period of five or more half-lives. The subject then receives a dose of the compound and blood samples are collected for pharmacokinetic or other analysis. The concentration of the dose is calculated to keep the subject’s exposure below the EDI. For this reason, it is important to establish the EDI before the clinical trial is designed and executed. After sufficient samples have been collected, the subject is released and the trial is complete for that subject. The subject then returns to a normal diet and levels increase again to levels similar to those before the study.

A pharmacokinetic study can be conducted below the EDI of EA. (Color figure online)
2 Assessment of EA Use
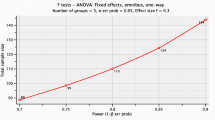
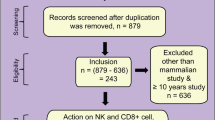
An assessment of the consumption of EA (EA) by the U.S. population resulting from the approved uses of EA was conducted. Estimates for the intake of EA were based on the approved food uses and maximum use level in conjunction with food consumption data included in the National Center for Health Statistics’ (NCHS) 2009–2010, 2011–2012, and 2013–2014 National Health and Nutrition Examination Surveys (NHANES) [27,28,29]. Calculations for the mean and 90th percentile intakes were performed for representative approved food uses of EA combined. The intakes were reported for these seven population groups:
-
1.
infants, age 0 to 1 year
-
2.
toddlers, age 1 to 2 years
-
3.
children, ages 2 to 5 years
-
4.
children, ages 6 to 12 years
-
5.
teenagers, ages 13 to 19 years
-
6.
adults, ages 20 years and up
-
7.
total population (all age groups combined, excluding ages 0–2 years).
3 Food Consumption Survey Data
3.1 Survey Description
The most recent National Health and Nutrition Examination Surveys (NHANES) for the years 2013–2014 are available for public use. NHANES are conducted as a continuous, annual survey, and are released in 2-year cycles. In each cycle, approximately 10,000 people across the U.S. complete the health examination component of the survey. Any combination of consecutive years of data collection is a nationally representative sample of the U.S. population. It is well established that the length of a dietary survey affects the estimated consumption of individual users and that short-term surveys, such as the typical 1-day dietary survey, overestimate consumption over longer time periods [30]. Because two 24-h dietary recalls administered on 2 non-consecutive days (Day 1 and Day 2) are available from the NHANES 2003–2004 and 2013–2014 surveys, these data were used to generate estimates for the current intake analysis.
The NHANES provide the most appropriate data for evaluating food-use and food-consumption patterns in the United States, containing 2 years of data on individuals selected via stratified multistage probability sample of civilian non-institutionalized population of the U.S. NHANES survey data were collected from individuals and households via 24-h dietary recalls administered on 2 non-consecutive days (Day 1 and Day 2) throughout all 4 seasons of the year. Day 1 data were collected in-person in the Mobile Examination Center (MEC), and Day 2 data were collected by telephone in the following 3 to 10 days, on different days of the week, to achieve the desired degree of statistical independence. The data were collected by first selecting Primary Sampling Units (PSUs), which were counties throughout the U.S. Small counties were combined to attain a minimum population size. These PSUs were segmented and households were chosen within each segment. One or more participants within a household were interviewed. Fifteen PSUs are visited each year. For example, in the 2009–2010 NHANES, there were 13,272 persons selected; of these 10,253 were considered respondents to the MEC examination and data collection. 9754 of the MEC respondents provided complete dietary intakes for Day 1 and of those providing the Day 1 data, 8,405 provided complete dietary intakes for Day 2. The release data does not necessarily include all the questions asked in a section. Data items may have been removed due to confidentiality, quality, or other considerations. For this reason, it is possible that a dataset does not completely match all the questions asked in a questionnaire section. Each data file has been edited to include only those sample persons eligible for that particular section or component, so the numbers vary.
In addition to collecting information on the types and quantities of foods being consumed, the NHANES surveys collected socioeconomic, physiological, and demographic information from individual participants in the survey, such as sex, age, height and weight, and other variables useful in characterizing consumption. The inclusion of this information allows for further assessment of food intake based on consumption by specific population groups of interest within the total population.
Sample weights were incorporated with NHANES surveys to compensate for the potential under-representation of intakes from specific population groups as a result of sample variability due to survey design, differential non-response rates, or other factors, such as deficiencies in the sampling frame [28, 29].
3.2 Methods
Consumption data from individual dietary records, detailing food items ingested by each survey participant, were collated by computer in Matlab and used to generate estimates for the intake of EA by the U.S. population. Estimates for the daily intake of EA represent projected 2-day averages for each individual from Day 1 and Day 2 of NHANES data; these average amounts comprised the distribution from which mean and percentile intake estimates were produced. Mean and percentile estimates were generated incorporating sample weights in order to provide representative intakes for the entire U.S. population. “All-user” intake refers to the estimated intake of EA by those individuals consuming food products containing EA. Individuals were considered users if they consumed 1 or more food products containing EA on either Day 1 or Day 2 of the survey.
3.3 Food Data
Food codes representative of each approved use were chosen from the Food and Nutrition Database for Dietary Studies (FNDDS) for the corresponding biennial NHANES survey. In FNDDS, the primary (usually generic) description of a given food is assigned a unique 8-digit food code [28, 29].
3.4 Food Survey Results
The estimated “all-user” total intakes of EA from all approved food uses of EA in the U.S. by population group is summarized in Figs. 2, 3, 4 and 5.

Children consume more EA on average than adults. Baby foods are often made from ingredients high in EA. The blue line shows data from the 2009–2010 NHANES, the red line data from the 2011–2012 NHANES, and the green line data from the 2013–2014 NHANES. (Color figure online)

Teenagers contribute the highest peak in the 90th percentile consumers of EA. The blue line shows data from the 2009–2010 NHANES, the red line data from the 2011–2012 NHANES, and the green line data from the 2013–2014 NHANES. (Color figure online)

When EA exposure is calculated on a per kilogram of body weight basis, toddlers aged 1 to 2 years are exposed to the most EA on average. The blue line shows data from the 2009–2010 NHANES, the red line data from the 2011–2012 NHANES, and the green line data from the 2013–2014 NHANES. (Color figure online)

When EA exposure is calculated on a per kilogram of body weight basis for the 90th percentile consumers, toddlers aged 1 to 2 years are again exposed to the most EA. The blue line shows data from the 2009–2010 NHANES, the red line data from the 2011–2012 NHANES, and the green line data from the 2013–2014 NHANES. (Color figure online)
The estimated “all-user” total intakes of EA from all approved food uses of EA in the U.S. by population group are graphed using NHANES data in Figs. 2, 3, 4 and 5 for 2009–2010, 2011–2012, and 2013–2014. The figures show that over 6 years, the consumption of EA has been fairly constant and that children and teenagers are the major consumers.
4 Conclusions
In summary, 28.3% of the total U.S. population of 2+ years was identified as consumers of EA from the approved food uses in the 2013–2014 survey. The mean intakes of EA by all EA consumers age 2+ (“all-user”) from all approved food uses were estimated to be 69.58 μg/person/day or 1.05 μg/kg body weight/day. The heavy consumer (90th percentile all-user) intakes of EA from all approved food-uses were estimated to be 258.33 μg/person/day or 3.89 μg/kg body weight/day. The EDI (red line in Fig. 1) is set at 70 μg/person/day from the 2013-2014 NHANES for consumers ages 2 and up. The next experiment will be an actual trial of EA in human subjects at the EDI with a dose of 3.89 μg/kg body weight/day (see Fig. 1), as determined by this DDCS study.
5 Support
The project described was supported in part by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1TR001998. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. This project was also supported by NSF ACI-1053575 allocation number BIO170011.
References
Park, S., Kang, Y.: Dietary ellagic acid suppresses atherosclerotic lesion formation and vascular inflammation in apoE-deficient mice. FASEB J. 27(1), 861-23 (2013)
García-Niño, R.W., Zazueta, C.: Ellagic acid: pharmacological activities and molecular mechanisms involved in liver protection. Pharmacol. Res. 97, 84–103 (2015)
Kaur, P., Thiruchelvan, M., Lee, R.C.H., Chen, H., Chen, K.C., Ng, M.L., Chu, J.J.H.: Inhibition of chikungunya virus replication by harringtonine, a novel antiviral that suppresses viral protein expression. Antimicrob. Agents Chemother. 57(1), 155–167 (2013)
Cerdá, B., et al.: Identification of urolithin A as a metabolite produced by human colon microflora from ellagic acid and related compounds. J. Agric. Food Chem. 53(14), 5571–5576 (2005)
Cerdá, B., et al.: The potent in vitro antioxidant ellagitannins from pomegranate juice are metabolised into bioavailable but poor antioxidant hydroxy–6H–dibenzopyran–6–one derivatives by the colonic microflora of healthy humans. Eur. J. Nutr. 43(4), 205–220 (2004)
Cerdá, B., Tomás-Barberán, F.A., Espín, J.C.: Metabolism of antioxidant and chemopreventive ellagitannins from strawberries, raspberries, walnuts, and oak-aged wine in humans: identification of biomarkers and individual variability. J. Agric. Food Chem. 53(2), 227–235 (2005)
Espín, J.C., et al.: Iberian pig as a model to clarify obscure points in the bioavailability and metabolism of ellagitannins in humans. J. Agric. Food Chem. 55(25), 10476–10485 (2007)
Mertens-Talcott, S.U., et al.: Absorption, metabolism, and antioxidant effects of pomegranate (Punica granatum L.) polyphenols after ingestion of a standardized extract in healthy human volunteers. J. Agric. Food Chem. 54(23), 8956–8961 (2006)
Seeram, N.P., Lee, R., Heber, D.: Bioavailability of ellagic acid in human plasma after consumption of ellagitannins from pomegranate (Punica granatum L.) juice. Clin. Chim. Acta 348(1), 63–68 (2004)
Seeram, N.P., et al.: Pomegranate juice ellagitannin metabolites are present in human plasma and some persist in urine for up to 48 hours. J. Nutr. 136(10), 2481–2485 (2006)
Tomás-Barberan, F.A., Espín, J.C., García-Conesa, M.T.: Bioavailability and metabolism of ellagic acid and ellagitannins. Chem. Biol. Ellagitannins 7, 293–297 (2009)
González-Barrio, R., et al.: UV and MS identification of urolithins and nasutins, the bioavailable metabolites of ellagitannins and ellagic acid in different mammals. J. Agric. Food Chem. 59(4), 1152–1162 (2011)
Espín, J.C., et al.: Biological significance of urolithins, the gut microbial ellagic acid-derived metabolites: the evidence so far. Evid. Based Complement. Altern. Med. 2013, 1–15 (2013)
Larrosa, M., et al.: Anti-inflammatory properties of a pomegranate extract and its metabolite urolithin-A in a colitis rat model and the effect of colon inflammation on phenolic metabolism. J. Nutr. Biochem. 21(8), 717–725 (2010)
Ishimoto, H., et al.: In vivo anti-inflammatory and antioxidant properties of ellagitannin metabolite urolithin A. Bioorg. Med. Chem. Lett. 21(19), 5901–5904 (2011)
Piwowarski, J.P., et al.: Role of human gut microbiota metabolism in the anti-inflammatory effect of traditionally used ellagitannin-rich plant materials. J. Ethnopharmacol. 155(1), 801–809 (2014)
Adams, L.S., et al.: Pomegranate ellagitannin–derived compounds exhibit antiproliferative and antiaromatase activity in breast cancer cells in vitro. Cancer Prevent. Res. 3(1), 108–113 (2010)
Seeram, N.P., et al.: In vitro antiproliferative, apoptotic and antioxidant activities of punicalagin, ellagic acid and a total pomegranate tannin extract are enhanced in combination with other polyphenols as found in pomegranate juice. J. Nutr. Biochem. 16(6), 360–367 (2005)
Seeram, N.P., Aronson, W.J., Zhang, Y., Henning, S.M., Moro, A., Lee, R.P., Sartippour, M., Harris, D.M., Rettig, M., Suchard, M.A., Pantuck, A.J.: Pomegranate ellagitannin-derived metabolites inhibit prostate cancer growth and localize to the mouse prostate gland. J. Agric. Food Chem. 55(19), 7732–7737 (2007)
Larrosa, M., et al.: Urolithins, ellagic acid-derived metabolites produced by human colonic microflora, exhibit estrogenic and antiestrogenic activities. J. Agric. Food Chem. 54(5), 1611–1620 (2006)
Liu, W., et al.: Pomegranate phenolics inhibit formation of advanced glycation endproducts by scavenging reactive carbonyl species. Food Funct. 5(11), 2996–3004 (2014)
Bialonska, D., et al.: Urolithins, intestinal microbial metabolites of pomegranate ellagitannins, exhibit potent antioxidant activity in a cell-based assay. J. Agric. Food Chem. 57(21), 10181–10186 (2009)
Giménez-Bastida, J.A., et al.: Urolithins, ellagitannin metabolites produced by colon microbiota, inhibit quorum sensing in Yersinia enterocolitica: phenotypic response and associated molecular changes. Food Chem. 132(3), 1465–1474 (2012)
González-Barrio, R., et al.: Bioavailability of anthocyanins and ellagitannins following consumption of raspberries by healthy humans and subjects with an ileostomy. J. Agric. Food Chem. 58(7), 3933–3939 (2010)
Tomás-Barberán, F.A., et al.: Ellagic acid metabolism by human gut microbiota: consistent observation of three urolithin phenotypes in intervention trials, independent of food source, age, and health status. J. Agric. Food Chem. 62(28), 6535–6538 (2014)
Truchado, P., et al.: Strawberry processing does not affect the production and urinary excretion of urolithins, ellagic acid metabolites, in humans. J. Agric. Food Chem. 60(23), 5749–5754 (2011)
CDC 2006: Analytical and Reporting Guidelines: The National Health and Nutrition Examination Survey (NHANES). National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, Maryland. http://www.cdc.gov/nchs/data/nhanes/nhanes_03_04/nhanes_analytic_guidelines_dec_2005.pdf
USDA 2012: What We Eat In America (WWEIA), NHANES: overview. http://www.ars.usda.gov/Services/docs.htm?docid=13793#release. Accessed 29 Jan 2018
Bodner-Montville, J., Ahuja, J.K.C., Ingwersen, L.A., Haggerty, E.S., Enns, C.W., Perloff, B.P.: USDA food and nutrient database for dietary studies: released on the web. J. Food Compos. Anal. 19(Suppl. 1), S100–S107 (2006)
Hayes, A.W., Kruger, C.L. (eds.): Hayes’ Principles and Methods of Toxicology, 6th edn, p. 631. CRC Press, Boca Raton (2014)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Dickerson, C., Ensor, M., Lodder, R.A. (2018). Establishing EDI for a Clinical Trial of a Treatment for Chikungunya. In: Shi, Y., et al. Computational Science – ICCS 2018. ICCS 2018. Lecture Notes in Computer Science(), vol 10861. Springer, Cham. https://doi.org/10.1007/978-3-319-93701-4_61
Download citation
DOI: https://doi.org/10.1007/978-3-319-93701-4_61
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-93700-7
Online ISBN: 978-3-319-93701-4
eBook Packages: Computer ScienceComputer Science (R0)