
Abstract
Scoliosis classification is useful for guiding the treatment and testing the clinical outcome. State-of-the-art classification procedures are inherently unreliable and non-reproducible due to technical and human judgmental error. In the current diagnostic system each examiner will have diagrammatic summary of classification procedure, number of scoliosis curves, apex level, etc. It is very difficult to define the required anatomical parameters in the noisy radiographs. The classification system demands automatic image understanding system. The proposed automated classification procedures extracts the anatomical features using image processing and applies classification procedures based on computer assisted algorithms. The reliability and reproducibility of the proposed computerized image understanding system are compared with manual and computer assisted system using Kappa values.
Similar content being viewed by others
Introduction
Scoliosis is a three dimensional deformity of the human spine in which there is one or more lateral curvature away from the vertical direction in the thoracic or lumbar region. The analysis of scoliosis is required through clinical and radiographic evaluation to fully assess the three dimensional deformity. Classification system for scoliosis serve the three main functions: categorization into recognizable and distinct group, prediction of natural history and prognosis and surgical as well as non surgical treatment [1]. Classification system used to guide the management of scoliosis should be reliable and each classification should relate to different prognosis or management strategy. State-of-the-art classification procedure are manual and computer assisted techniques which relies on radiographic measure are used in surgical planning for patient with scoliosis [7].
The association of radiographic classification with clinical findings can begin to address the ultimate goal of classification system by guiding both surgical and non surgical treatment. Scoliotic curve pattern classifications, that rely on radiographic measure are used in surgical planning for patient with scoliosis [7, 12]. The curve were counted and classified into single, double and triple curves to the apex number.
Surgical intervention is generally required, if spinal deformities are severe or progressive. For the single curve, such as thoracic, thoraco-lumbar or lumbar curve, there are few differences in the selection of fusion level among different spinal surgeons except for surgical approaches. However, the choice of fusion level in some types of curve, such as double curves remains different and controversy issue [4]. Inadequate fusion in these curves may result in postoperative curvature deteriorations, trunk decomposition or can produce new deformity. The selection of approach and fusion level should be based on the inherent characteristic of different curves. A good classification system has to include different types of the curves and should be a guide for a surgical planning.
There are currently two recognized classification methods, viz., King Classification [4] and Lenke classification [6]. King classification has 5 patterns and Lenke has 42 potential patterns. The King’s classification method helps to decide the level of fusion and instrumentation on the spine of the scoliosis patient [4].
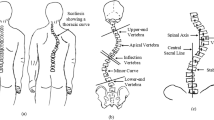
The classification by King is still the most widely used technique in surgical planning. It defines 5 thoracic curve types and an identical group called miscellaneous. The King classification relies on subjective identification and measurement of radiographic features including the apical and end vertebra of the curve, vertebral end plate and origin of alignment of the central sacral line(CSL). The King’s classification definition follows as below (refer Fig. 1).
-
King Type I: Shows an S-shaped curve crossing the mid line of the thoracic and lumbar curves. The lumbar curve is larger and more rigid than the thoracic curve.
-
King Type II: Shows an S-shaped curve where both the thoracic major curve and the lumbar minor curve cross over the mid line. The thoracic curve is the largest curve.
-
King Type III: Shows a thoracic curve where the lumbar curve does not cross the mid line.
-
King Type IV: Shows a long thoracic curve where the 5th lumbar vertebra is centered over the sacrum, but the 4th lumbar vertebra is already angled in the direction of the curve.
-
King Type V: Shows a thoracic double curve where the 1st thoracic vertebra angles into the convexity of the upper curve.

Kings classification (A) Type-I (B) Type-II (C) Type-III (D) Type-IV (E) Type-V (Source:American Association of Neurological Surgeons)
Classification of scoliosis not only organizes an approach to a problem, it also supports a method of treatment and provides an estimate of particular treatment. State-of-the-art systems for classification are manual [4] and computer assisted technique [6, 10, 11]. In case of manual method, the parameters are manually quantified by observation and angle is calculated using ruler and pencil procedure. Each reviewer was provided with diagrammatic summary of the five types of curve according to the classification system. Manual procedure needs number of scoliosis curve, each should be identified by the apex level, end vertebra and Cobb angle [2, 5]. The position of the certain vertebrae relative to plumb line and whether the lumbar curve and thoracic curves crossed the mid line are to be identified manually. The tilt of L4 and T1 and the elevation of the first rib and flexibility index are done with human judgments.
In case of computer assisted method, first step is to record the coordinates of defined landmark on radiographs. The digitized landmarks were four corners of the each vertebra from T1 to L5 and two symmetric landmarks on the proximal sacrum. In the computerized method they adopted the following procedure relating to the posterioanterior (PA) radiographs. The midpoint between the symmetric digitized points on the sacrum defined the origin of the patient in XY system. The CSL was defined as the vertical line passing through the origin. Centroid of the vertebral column described the medial axis. The classification is based on the displacements between medial axis and the CSL with the assistance of computer [10, 11].
State-of-the-art classification system relies on subjective identification and measurement of the radiographic features. It also requires individual interpretation and memorizing the classification criteria. But the computer assisted methods reliability is influenced by experience of individual who is using the tool, magnitude of scoliosis and quality of image. From the literature it was reported that classification is unreliable when a radiographic measurement was close to the threshold value used to distinguish between curves of two different types.
The scoliosis classification procedure demands an automatic system for identification of number of curves, curvature parameter [3] and required vertebral end plates. Thereby subjectivity involved in classification can be drastically reduced. This paper proposes a technique for automatic identification of these parameters using image processing algorithms followed by computer assisted system.
The proposed method extracts the ROI using the image flipping operation. The flipped version of the image is fed to the segmentation method with gray level reference, that results in segmented vertebral column. The CSL and medial axis are found using this vertebral boundary. These two will be the main source of information to know the extent of deviation of the curve in various regions. In turn these deviations are fed to a classification system which satisfies King’s definition to classify them into one of the five categories.
Literature review
Classification procedure that rely on radiographic measure are used in surgical planning for patient with idiopathic scoliosis. The King classification relies on subjective identification and measurement of the radiographic features, including the apical and end vertebrae and vertebral end plate tilt. Errors in identifying these radiographic landmarks and using the resulting measurements in identifying the pattern of deformity provides numerous opportunities for both technical and judgmental errors, resulting in inter-and-intra- observer error.
In 1998 Lawrence et al. [6] has done a study to determine the reliability of the classification of thoracic adolescent idiopathic curves. They have a good team of 8 members from Scoliosis Research Society(SRS). Each reviewer was provided with diagrammatic summary of the five types of the curves according to the classification. This study had two shortcomings, first they have an overall reviewer bias as five of eight were members of a scoliosis study group and they have a different training background. Secondly the curves were pre-selected by the lead author because they had a difficulty in classifying themselves. Finally the mean inter observer reliability of the classification was only 64%, it is very poor.
In 2002 Ian et al. [11] has done a study to reduce or eliminate the sources of errors. The measurement used in classification includes end points, range of lateral bending and parameters relating to spinal alignment and vertebral tilt. The purpose of their study is to report whether radiograph of a patient with idiopathic scoliosis could be reliably classified by the King’s method using unambiguous rules for classification encoded in computer program. There are two steps in the encoded computer method, first is to record the coordinates of the defined landmark on the radiographs, to assist objective determination of the parameters used to distinguish between group and second step is to apply the rule. This computer assisted algorithm works automatically only under the condition that required coordinates of the landmarks are clearly defined. Defining the landmark on the noisy radiograph itself is a main source of error.
The most common problem in King’s classification is postoperative decomposition after selective thoracic fusion in King Type-II curves and comparative study among different institutes are eliminated because of its lower reliability and reproducibility. In 2005 Guixing et al. [8] defined a new classification system, which categorizes idiopathic scoliosis into 3 different types according to the number of curves, but it is a new classification system. SRS adopted King’s as the standard one. Further study on the reliability and reproducibility of this system at other spinal centers are needed.
In 2006 Ian et al. [10] continued their study on the reliability of the classification. In this study they want to check how much the above mentioned computer assisted algorithm is reliable. Their conclusion is that there is an influence of experience of the individual using computer assisted tool, magnitude of scoliosis and image quality.
In 2010 Rigo et al. [9] introduced a new classification system which will correlate with surgical treatment. They showed that proposed new classification has better inter-and-intra-observer reliability with brace treatment. But their new system needs human intervention in identifying the position of the transition point between thoracic curve and caudal curve along with its CSL.
Above study concludes that even manual and computer assisted classification system depends on quality of radiograph, severity of scoliosis and individual experience. There is a requirement of an automated system which uses computerized image understanding.
Methods
Materials
Posterioanterior radiographs of 150 patients with idiopathic scoliosis are used for study from Kasturba Medical College Manipal Karnataka India. These radiographs were taken in a conventional standing posture at a fixed distance of 228cm from X-ray source with knees fully extended and upper limbs resting on two arm support. These PA radiographs includes thoracic, thoraco lumbar and lumbar scoliosis with all classes of scoliosis as defined by King. For the present study, the radiographic images were presented in a gray scale with size 925 pixel height by 475 pixel wide.
Automatic scoliosis classification
The inter-and-intra-observer variation involved in classification of scoliosis can be completely eliminated by automatic identification of required anatomical parameters in the noisy radiographs. The parameters are number of curves, starting and ending point and steepness of the curve. This automation completely depends on the available spine boundary. Extracting the spine boundary from noisy radiograph involves various image processing techniques.
The proposed research uses global, local and adaptive threshold technique. First step is to isolate the spine boundary from the given radiographs. This isolation depends on the image content as it has deviation in both left and right side of its central spine axis. Due to nature of the scoliotic spine it is difficult to predict the orientation of the vertebral column in right and left side. This can be accomplished by adding the flipped version of the image with its original version along the spine axis. The extracted ROI still contains extraneous information such as rib cabs, pelvic region, etc. This can be eliminated by applying FFT interpolation for row wise gray level profiles.
Figure 2 shows different imaging techniques used in extracting vertebral column from a given radiographs. The first pre-processing step is to add the original image (Fig. 3a) with its up-down flipped version (Fig. 3b), results in an image shown in Fig. 3c. The maximum gray level value is chosen as the first global threshold value. The resultant image will be black and white image with white pixel region enveloping a minimal extraneous content as shown in Fig. 3d. A bitwise logical AND operation has been applied to retrieve back the original X-ray features localized to the enveloping region as shown in Fig. 3e. Matrix-to-row converter is used to extract the expected rows from the image. The row-wise gray level profiles have noisy component accompanying the gray levels of the ROI. These noisy components are like spike in nature which makes the gray level thresholding decision cumbersome. Hence prior to application of thresholding these gray level profiles are fed to the interpolation technique.

Block diagram for extraction of vertebral column

(a) Input image (b) Flipped version of input image (c) Image after arithmetic addition operation (d) Image after thresholding (e) Image after logical AND operation (f) Extracted ROI
There are two different types of interpolation namely polynomial based and FFT based. The polynomial interpolations requires the data to be monotonic. The given gray level profiles are neither monotonically increasing nor decreasing. The FFT based interpolation is independent of sample data. Hence resultant gray level profiles are subjected to FFT interpolation technique. Figure 4a graph shows the comparison between gray level profiles of one row of an image after bit-wise logical AND operation with its interpolated version. Figure 4b graph shows the partial suppression of the extraneous information by adding the original row level profiles with the interpolated version. Now a threshold value can be directly set without extraneous information as shown in Fig. 4c graph. This thresholding technique gives ROI as shown in Fig. 3f.


Gray level Profiles (a) Original gray level profile with its interpolated version (b) Partial suppression by adding original with interpolation (c) Desired ROI’s gray level profiles
Medial axis and central sacral line:
Computer assisted scoliosis classification are based on the deviation of the spine axis from the CSL and other aspect such as existence of double thoracic and single thoracic curves on the same or different side. As explained in introduction computer assisted system defines CSL and medial axis using 70 manually identified landmarks. Automatic extraction of CSL and medial axis in case of computerised image understanding system are explained below.
Segmentation procedure results in extraction of the vertebral column as shown in Fig. 3f. A boundary operation is performed on the extracted vertebral column using erosion technique. The boundary representation consists of pair of coordinates. Subsequently extract the medial axis from these boundary co-ordinates. For every co-ordinates there exists two X-values. The average of these two X-values will be the X-coordinates of the medial axis. CSL is a vertical line representing the global axis, and it is drawn from the center of the upper end plate of S1.
The medial axis and CSL obtained acts as a input to the proposed classification technique as shown in Fig. 5. It finds the deviation between these two MA and CSL. This deviation is used to identify the category of classification. The rule applied is, if the MA cross the CSL twice, it is categorized category-1 otherwise category-2. The category-1 consists of Type-I and Type-II and category-2 consists of Type-III,Type-IV and Type-V. In category-1 if the first level deviation is more than the second level, then it is categorized into Type-I otherwise Type-II as shown in Fig. 5. Under category-2, if the centroid of the medial axis has the maximum deviation, then it is classified as Type-V with one curve with maximum deviation at the center. If the medial axis crosses the CSL once without having the maximum deviation at the center along with the upper region MA and CSL are parallel then categorized into Type-III otherwise Type-IV.

Proposed classification technique using medial axis and central sacral line
Results
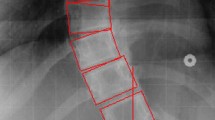
Radiographic features used for computer assisted classification of scoliosis are medial axis and CSL. It requires 70 landmark identification at the corners of 17 vertebral body starting from T1 to L5. The proposed computerised image understanding system automatically defines medial axis and CSL with the help of image processing techniques. Medial axis is embedded within the vertebral column. Different thresholding techniques are applied to select proper ROI from the posterioanterior radiographs. The resultant vertebral columns are shown in Fig. 6b. Determination of medial axis needs only the boundary coordinates. These boundary coordinates are retained using boundary descriptors as shown in Fig. 6c. Coordinates of the spine axis are nothing but the average coordinates of the boundary in X- axis. CSL is nothing but the vertical line drawn from the center point of the L5 vertebra. Figure 6d shows the medial axis and mid line for the classification procedure.

Different classes of scoliosis (a) Input radiograph (b) Segmented vertebral column (c) Extracted boundary (d) Classified output with MA and CSL
Discussions
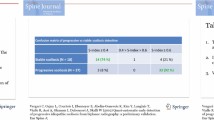
Inter and intra observer reliability among 5 examiners at 4 different intervals were presented in Table 1 for different King’s type each with a minimum of 10 radiographs per group. Table 1 represents the consistency ratio and its corresponding Kappa value for different classification procedures (manual, computer assisted and computerized image understanding). The consistency is very poor in the manual method compared to computer assisted and computerized image understanding. The clinical interpretation of Kappa (κ) values are summarized using bounding values as follows: slight agreement between κ=0.00 and 0.20, fair between κ=0.21 and 0.40, moderate between κ=0.41 and 0.60, substantial between κ=0.61 and 0.80, and almost perfect between κ=0.81 and 1.00.
In the manual classification procedure, each examiner has to remember the classification definition by King and he has to find the required parameters as mentioned in the requirements. It includes the manual calculation of Cobb angle and definition of vertebral end plates. If the examiner fails in defining the vertebral end plates, that error will be propagated to classification procedure. Other indexing parameter also depends on the landmark identification procedure. Landmark identification on radiograph is a tedious process, also varies from person to person and time to time. Hence the consistency is in the moderate range.
The computer assisted method depends on digitized 70 landmarks. The consistency ratio is in the reliable range. Here all the manually identified landmark on digital radiographs needs human intervention, remaining steps follows computer assisted methods. The Kappa statistics for this methodology lies between moderate(<0.6) and substantial range (0.7).
Computerized image understanding system, first extracts the features as required for the computer assisted technique by the examiner. For extraction, image processing technique is used without any human intervention. The required landmarks are automatically (coordinates points for medial axis and CSL coordinates) recorded as its coordinate points. The classification procedure needs number of curves and its deviation at different stages. That is quantified by displacement of the medial axis from its CSL. This will categorize radiographs into different types as per the King’s definition. For the moderate curve range, the consistency ratio and Kappa value both are in good range. As a special case curve with more severity (>50), the defined Gaussian filter in the ROI selection may not work with full accuracy, under such situation one may have to increase the filter range. This increase in the filter range highlights unwanted region as rib cabs and pelvis region. Removal of noise may work up to some extent not of the required level. The Kappa statistics for proposed methodology falls between substantial and perfect range. The proposed system shows better classification consistency compared to manual and computer assisted. Landmark identification in case of manual and computer assisted system are time consuming and it needs expert radiologist. In the proposed research the observer doesn’t require any training in the classification procedure and manual landmarking is completely avoided. Still there is some consistency deficiency due to presence of noise in the radiographs. During the extraction of the vertebral column due to noisy nature of X-ray, one may have to select higher value for the Gaussian filter. This higher value leads to more extraneous information in the selected ROI. This minor error may cause misclassification, but works well compared to existing system.
References
Nader, M. H., and Tortolani, P.J., Idiopathic scoliosis in adults classification indications and treatment options. Spine surg. 21:16–23, 2008.
Michelle, C., Tanure, A., Pinheiro, P., Oliveira, A. S., Technical report reliability assessment of Cobb angle measurements using manual and digital methods. Spine J. 10 (9):769–774, 2010.
Anitha, H., and Prabhu, G. K., Automatic quantification of spinal curvature in scoliotic radiograph using image processing. J. Med. Syst. 36 (3):1943–1951, 2012.
King, H. A., Moe, J. H., Bradford, D. S., The selection of fusion levels in thoracic idiopathic scoliosis. J. Bone Joint Surg. 65 (9):1302–1313, 1983.
Kuklo, T. R., Potter, B. K., WPolly Jr, D., O’Brien, M. F., Schroeder, T. M., Lenke, L. G., Reliability analysis for manual adolescent idiopathic scoliosis measurements. Spine 15:30 (4):444–454, 2005.
Lenke, L. G., Betz, R. R., Bridwell, K. H., Clements, D. H., Harms, J., Lowe, T. G., Shufflebarger, H. L., Intra observer and inter observer reliability of the classification of thoracic adolescent idiopathic scoliosis. J. Bone Joint Surg. 80a (8):1097–1106, 1998.
Malfair, D., Flemming, A. K., Marcel, F., Dvorak, P., Alexander, Identification of spinal deformity classification with total curvature analysis and artificial neural network. Radiographic Eval. scoliosis Rev. 194 (3): S8–22, 2010.
Qiu, G., Zhang, J., Wang, Y., Xu, H., Zhang, J., Weng, X., Jin, L., Yu, Z., Shen, J., Yang, X., Luk, K., LU, D., Lu, W., A new operative classification of idiopathic scoliosis: A peking union medical college method. Spine 30 (24):1419–1426, 2005.
Rigo, M. D., Villagrasa, M., Gallo, D., A specific scoliosis classification correlating with brace treatment: description and reliability. Vol. 5, 2010.
Stokes, I.A.F., and Aronsson, D.D., Computer assisted algorithms improve reliability of king classification and Cobb angle measurement of scoliosis. Spine 31 (6):665–670, 2006.
Stokes, I. A. F., and Aronsson, D. D., Identifying sources of variability in scoliosis classification using a rule-based automated algorithm. Spine 27 (24):2801–2805, 2002.
Zhang, J., Lou, E., Hill, D. L., Raso, J. V., Wang, Y., Lawrence, H., Le, X. S., Computer aided assessment of scoliosis on posterior radiographs. Med. Biol. Eng. Comput. 48:185–195, 2010.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Systems-Level Quality Improvement
Rights and permissions
About this article

Cite this article
Anitha, H., Prabhu, G.K. & Karunakar, A.K. Reliable and Reproducible Classification System for Scoliotic Radiograph using Image Processing Techniques. J Med Syst 38, 124 (2014). https://doi.org/10.1007/s10916-014-0124-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-014-0124-z