Abstract
Background
Acquired brain injuries are one of the main causes of human disability worldwide. It can lead to social isolation due to physical and mental dysfunctions. Studies on using robots in social psychiatry have shown positive results regarding mental function and social behavior among patients facing challenges similar to acquired brain injury (ABI).
Aim
To explore how the telepresence avatar robot OriHime can be used as a communication tool between patients at home with mild-to-moderate ABI and members at a rehabilitation center with ABI and to determine whether the telepresence avatar robot OriHime can motivate the patients at home to participate in rehabilitation activities at the rehabilitation center.
Method
We conducted an exploratory ethnographic case study, applying the conceptual framework ‘community of practice.’ The intervention consisted of sessions where ABI patients at home (n = 8) interacted with a member (n = 4) from Aalborg Rehabilitation Club using OriHime. Data collection consisted of documentary materials, participant observation (141 h) and semi-structured interviews (n = 11). The data were analyzed and triangulated in NVivo 12.0.
Findings
The patients at home found nonverbal communication valuable, while the members at the rehabilitation center felt that OriHime lacked human features and preferred direct verbal communication. The technology facilitated a feeling of being a part of a community of practice between the participants, and it motivated the patients at home to participate in the rehabilitating activities. One patient visited the rehabilitation center physically.
Conclusion
OriHime can as a communication tool motivate and engage patients to participate in rehabilitating activities.
Similar content being viewed by others



1 Introduction
An increasing number of people worldwide are suffering from an acquired brain injury (ABI), most commonly caused by strokes or traumatic incidents [1, 2]. Strokes and traumatic brain injuries are one of the main causes of death and human disability worldwide [1, 2]. In 2013, the annual incidence of mortality due to stroke was 10.3 million [2], while it is estimated that 69 million persons suffered a traumatic brain injury in 2018, of whom 81% would experience in a mild brain injury [1]. ABI patients who survive the incident usually have to live the rest of their lives with a variety of physical and/or mental disorders [3,4,5]. This can lead to a loss of mental functions such as awareness disorders, change in behavior and depression [3,4,5], all of which are partly caused by negative psychosocial behavior such as isolation [3]. ABI can also manifest itself as fatigue, memory disorders, aphasia, epilepsy and paralysis of one side of the body or a limb [3, 6, 7]. Additionally, ABI patients perception of how other people perceive them makes them feel abnormal [8] and handicapped [9], resulting in feelings of insecurity, loss of friendships [8] and unemployment [5]. ABI patients’ lack of participation in social activities can result in isolation tendencies [3], and the risk of mortality due to suicide among people with an ABI is twice as high as the general population [10].
A case study, review and a meta-analysis indicate that community-based efforts for people with an ABI should be included as a tool for supporting and easing the rehabilitation process [1, 8].
Reviews [11, 12] also highlight that rehabilitation for patients with an ABI has shown positive effect on cognitive functions, mental health and activities of daily living (ADL), if these measures include social activities within a community, such as leisure activities and job-related activities supported by health professionals [11, 12]. Knowledge shared with to the ABI patients about their illness and how to ease ADL problems has been shown to reduce their symptoms of depression and improve their psychosocial state of mind [11]. Social interaction is also an important part of rehabilitation for those with ABI. Social interactions give the ABI patient a more positive attitude toward themselves and others, as well as facilitating their sense of belonging in a community, all of which enhances their learning process [7, 13, 14].
Within the field of social psychiatry, treatment of illness, such as depression, has relied on pharmaceuticals [15]. However, because drug-based treatment risks dangerous side effects [15], recent research has begun to look to the field of robot solutions as a potential alternative to pharmaceuticals [15].
1.1 Robots in social psychiatry
Robots have shown promising results in older adults suffering from depression, dementia and cognitive impairment [15,16,17,18]. Although the results have not been considered statistically significant, the general trends have been positive regarding patients’ acceptance of the robot, independence, quality of life, depression, anxiety, loneliness, isolation, improved brain activity, memory and improved sleep pattern [15, 16, 18, 19]. Studies of social robot use also showed that patients became significantly more socially active, verbally and nonverbally [16]. The social robot PARO, for example, seemed to have had an impact on elderly persons with dementia, reducing their sense of loneliness, boredom, depression and making them more socially active [15, 16, 20]. Furthermore, use of humanoid robots have been shown to have a positive influence on elderly with dementia [21].
Telepresence robots have also shown a useful potential in improving the quality of life for elderly with dementia as they help maintain social connections and facilitate meaningful conversations, thus counteracting feelings of isolation [22].
The field of social robotics still lacks sufficient evidence of its effect on patients, and it is suggested that more studies with larger sample sizes are necessary [15,16,17,18]. According to our systematic literature search, we have not identified other studies that have explored the possibilities of utilizing telepresence avatar robots as a communications tool for patients with an ABI.
The aim of this paper was twofold: First is to explore how the telepresence avatar robot OriHime could be used as a communication tool between mentors (volunteers with an acquired brain injury at a rehabilitation center) and patients at home with a mild-to-moderate ABI. Second is to determine whether the telepresence avatar robot OriHime can motivate patients at home to participate more actively in rehabilitation activities.
2 Methods
2.1 Design
The study was designed as an exploratory single case study. A case study focuses on research of how and why a social phenomenon unfolds in its real-world context. As such, a case study is defined as ‘an empirical inquiry that investigates a contemporary phenomenon (the case) in depth and within its real-world context’ [23]. Within the case study, we used an ethnographic approach. Ethnography is a description of a human phenomenon and action that can be used to understand, interpret and describe social or cultural relationships [24]. To understand and describe the social phenomena, the ethnographer actively participates in people’s daily life for an extended period of time, a technique called ‘participant observation’ [24].
2.2 Ethical approval and considerations
The Danish Ethical Committee was contacted, and since the technology in our study was being used as a communication tool, the study did not have to be reported. Our study was performed according to the Declaration of Helsinki, and all participants signed an informed consent agreement. The data were processed accordingly to the General Data Protection Regulation [25], and Danish regulation requirements regarding privacy were also followed [26].
2.3 Presentation of the study context
2.3.1 The case
During the study, an OriHime robot was placed at Aalborg Rehabilitation Club (ARC) in Aalborg Municipality (Denmark). ARC, is a club for persons who have suffered a mild-to-moderate brain injury [27]. ARC is a user-driven organization established and founded by Aalborg Municipality. The club is managed by its members, who are supported by ARC employed staff [27]. Once a month, ARC has a ‘house meeting’ where members discuss the current state of club activities and suggest possible changes and management. Citizens pay no fee to becoming a member of ARC, and participation is both open and voluntary [27].
The aim of ARC is to maintain and develop the members’ physical and psychological functions and competencies as a preparation for future employment [27]. This is carried out through promotion of a healthy lifestyle that is achieved through a healthy diet, working on the individual’s well-being, socializing, ADL activities and physical exercise (walks, chair yoga, fitness) which members can sign up for at the daily morning meetings [27]. ADL activities in the club consist of administration/office work, writing job applications, household chores, cooking, creative activities (playing music, painting etc.), cognitive training and planning other activities or events [27].
2.3.2 The technology
The technology has been defined and redefined through adjustments during the study (Appendix 1). The final setup of the technology is described in the following:
-
The telepresence avatar robot OriHime (Fig. 1).
Fig. 1 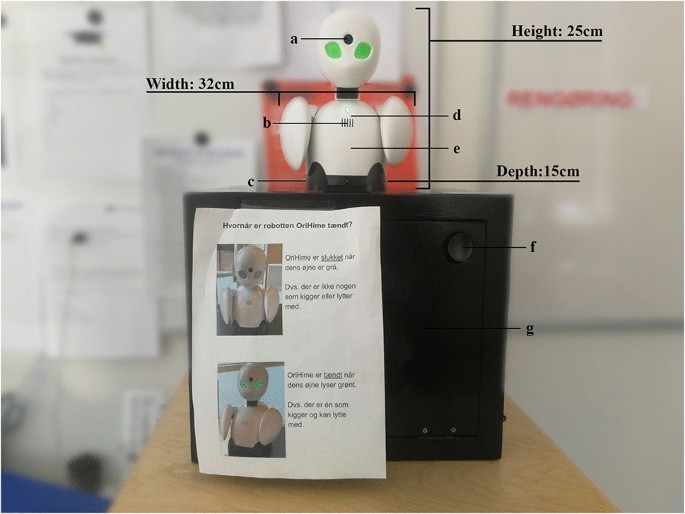
OriHime and the setup used in the study. Shown are a camera, b speaker, c power outlet, d microphone, e motor, f additional speakers, g computer (inside the box). The poster placed on the wooden box informs the members when OriHime is turned on/off
-
A computer connected to the internet, with OryLab’s software ‘OriHimeBiz v3.0.4.’
-
A USB cable to connect OriHime to the internet through the computer.
-
A USB cable from the power outlet to connect OriHime to a power source.
-
A tablet with ‘OriHime biz controller v1.33.0’ app and 4G connection.
-
A roller cabinet to make OriHime mobile.
-
A large wooden box to place OriHime at eye level and make it more practical (for storing the computer, cables and speakers).
-
Two additional speakers connected to the computer.

2.3.3 OriHime
OriHime is designed as a telepresence avatar robot. Its purpose is to help people engage in life-like social behavior over distance and to facilitate human-to-human social interaction as well as serving the purpose of being an avatar to the user [22, 28].
Patients at home with an ABI who are curious about ARC and its community have the possibility to use a tablet from their home and connect with OriHime. This could provide interaction with ARC’s members by using nonverbal communication through its predefined functions and/or verbal communication. Further, since OriHime functions as an avatar for the patient at home, it allows the patient to be anonymous.
As shown in Fig. 1, the dimension of OriHime is 25 × 32 × 15cm and its weight is 600 g. OriHimes motor enables the user of the tablet to control its head and arms individually by swiping left/right on the tablet or by using predefined functions in the app, such as ‘nod,’ ‘shake the head,’ ‘lift its arms in sign of applause’ or ‘O.K.’ OriHimes built-in camera can livestream HD video with a 103° wide angle. The robot’s built-in microphone and speaker makes bilateral verbal communication possible. In this study, additional speakers were used in order to enhance the sound quality and volume. OriHime was placed on a wooden box, within which the speakers and the computer were placed (Fig. 1). The entire OriHime assembly and speakers, together with the wooden box, was mounted on a roller cabinet to make it mobile and to achieve eye level contact.
2.4 Description of sampling
The participants included in the study had following characteristics: residents of Aalborg Municipality, Denmark; had a mild-to-moderate acquired brain injury; between the ages of 18 and 70 years; self-reliant in self-care. Mentors had to be a member of ARC. Participants were excluded if they had an alcohol/drug addiction; severe aphasia; inability to speak Danish or English (Table 1). The ABI patients at home were continuously recruited over the timespan of 5 months (Jan 2019–May 2019) by the social workers, ARC staff and by the investigating authors. In April 2019, four patients at home with an ABI were recruited, and in order to recruit additional patients for the study, we created a pamphlet, a video and a presentation to the social workers encouraging them to seek out potential patients.
In the study, a total of 13 participants were recruited. The participants were ABI persons living in their homes (n = 9) (ABI patients at home) and volunteer members at ARC (n = 4), who functioned as mentors for the ABI patients at home (mentors).
2.5 Description of the study process
Throughout the study, we used an ethnographic approach, taking part in ARC’s everyday life and visiting the participants in their homes during the intervention.
2.5.1 Phase 1: study preparation
As seen in phase 1 (Table 2), two meetings were held, where the study process was discussed among the participants of the meetings. In this phase, we obtained data from participant observation and documentary materials. The formal recruitment of the patients at home and mentors to the study was discussed and initiated. We also held a workshop for the social workers and ARC staff to provide details of the intervention and to introduce them to OriHime.
2.5.2 Phase 2: pilot testing
In phase 1 (Table 2), participant observation was carried out in order to explore the daily life at ARC and to gain knowledge about their community. In this phase, the members and mentors were slowly introduced to OriHime and given ample opportunity to ask questions, so mentors could feel more secure about their tasks and members could become familiar with the technology. To apply our explorative approach, the mentors and the staff at ARC were also given the opportunity to have an influence on the intervention.
We pilot tested the technology over distance and carried out multiple pilot tests at ARC in order to identify potential difficulties, after which we adjusted the intervention accordingly (Appendix 1). Other relevant adjustments were made based on inputs we received from ARC members and staff.
A third meeting was held, the purpose of which was to follow up on the study and resolve technical difficulties encountered during the pilot testing.
2.5.3 Phase 3: the intervention with OriHime
Prior to commencing the intervention, we held an individual introduction for the ABI patients at home (Table 2). They were introduced to OriHime so that they could get hands-on experience and feel more secure with the technology. Afterward, they could choose between sessions consisting of either experiencing the activities at ARC or a guided tour through OriHime managed by a mentor and sometimes assisted by an ARC staff, if available.
As seen in Figs. 2, 3 and 4, the intervention consisted of sessions with the ABI patients at home who are using an app for the OriHime on a tablet so that they were able to see and talk with the mentors at ARC as well as control the movements of OriHimes head and arms. The ABI patient at home was able to view the environment at ARC and could choose to be taken on a guided tour of the rehabilitation centers main floor, where most of the ADL activities took place, and/or in the basement, which offered more creative activities. The activities offered to the participant included morning meetings, ADL activities, social activities or creative activities led by either a mentor or an ARC member (Fig. 5).

The ABI patient at home controlling OriHime with an iPad and thereby interacts with a mentor at ARC


An ABI patient at home interacting with a mentor at the rehabilitation center by controlling OriHime with an iPad

An ABI patient at home interacting with a mentor, member and ARC staff through OriHime during one of the creative activities at ARC
The patients at home could schedule as many sessions with the intervention as they wished, until they wanted to cease participating in the study, decided to visit ARC in person or until the end of the data collection period.
The mentor in charge of the session was either chosen beforehand or contacted on the same day during the morning meetings. The patients at home did not have a specific mentor assigned to them, such that they could have different mentors for each session. During this phase, we held a second workshop with the social workers and ARC staff in order to discuss current experiences with OriHime and how OriHime should be used in the intervention.
2.5.4 Phase 4: interviews
In the final phase (Table 2) of our study, we interviewed the ABI patients at home after their final session of the intervention, while the interviews with the mentors were held at the end of the whole intervention period.
2.6 Theoretical framework
In this study, we applied Wenger’s learning theory approach, known as ‘community of practice’ because according to the literature it is important for patients with an ABI to be a part of a community and share their experiences as it enhances their psychosocial well-being and learning processes [7, 11, 13, 14]. A community of practice is defined as ‘groups of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly’ [29, 30]. Every community of practice consists of three elements: community, domain and practice. A community of practice is bound by (Fig. 3) relations of trust that the members develop with each other so as to facilitate their learning [29].
The themes in the observational guide (Appendix 2) and interview guide (Appendices 3 and 4) were inspired by the theoretical framework.
The framework was translated into interview questions by asking questions such as ‘What was it like to speak with another person through OriHime?’ and ‘what did you talk about’ to explore if they were sharing experience about their ABI according to the framework, or ‘Would you like to become a member of ARC after using OriHime’ to explorer if being a part of a community of practice through OriHime would motivate the patients with ABI at home to join ARC. We also wanted to make the interview questions open and explorative taking their injury into account.
2.7 Data collection techniques
To explore the interaction with OriHime, we collected data in the form of documentary materials, participant observation and semi-structured interviews. The collected data were triangulated to improve validity [31].
2.7.1 Documentary materials
The aim of collecting documentary materials was to gain background and baseline data that would refine our theoretical approach to ARC [23] and better understand the characteristics of patients with an ABI in general. Documentary materials consisted of homepages, policy documents from Aalborg Municipality, and summaries of ARC ‘house meetings. The documents were analyzed using NVivo 12.0.
2.7.2 Participant observation
We constructed an observation guide (see Appendix 1) based upon the theoretical framework (see Appendix 1). The purposes of the guide were to (1) gather data about the community of practice at ARC, (2) observe the interaction between the ABI patients at home and their mentors through the technology, and (3) explore their perception of the technology.
The observations took place at ARC during the initial meetings with ARC staff and Aalborg Municipality, during the workshops with ARC staff and during the everyday activities of the members. Observations were also performed during the pilot tests of the technology at ARC as well as during the introduction and the intervention with the mentors and members at ARC and in the ABI patients’ homes.
A total number of 141 h of participant observation were carried out by the investigating authors.
Observational notes were taken when possible while the observations were taking place or immediately afterward, written in Microsoft Word and analyzed using NVivo 12.0.
2.7.3 Semi-structured interviews
We conducted semi-structured interviews [32] (n = 12) with the aim of exploring (1) the ABI patients at home and mentors’ experiences of the intervention and (2) their interaction with the technology. We developed an interview guide with key themes based on the community of practice framework (Appendices 3 and 4). We interviewed the mentors and the ABI patients at home after their final use of the technology.
The participants had to attend at least one session with the intervention before being interviewed. Of the total 12 interviews conducted, 8 were with ABI patients at home and 4 with the mentors. Interviews lasted between 11 and 38 min.
The interviews with the mentors took place in a closed and quiet office at the ARC, while interviews with the ABI patients took place in their homes.
The interviews were carried out individually by one of the investigating authors. They conducted four interviews each, all of which were audio recorded, then transcribed and analyzed in NVivo 12.0.
2.7.4 Data analysis
Data from the participant observation, semi-structured interviews and relevant documentary materials were imported and analyzed in NVivo 12.0 according to the approach of Brinkmann and Kvale [32]. All of the investigating authors participated in the analysis process, which was carried out in the following steps:
-
1.
Transcriptions from 3 interviews were read and coded individually by the investigating authors.
-
2.
To ensure intersubjectivity, the coding was discussed until the investigating authors obtained the same understanding of the themes.
-
3.
An initial code tree was determined for central themes from the theoretical framework and from themes identified in step 1.
-
4.
All data were analyzed, and if new themes were identified, they were added to the node tree in NVivo 12.
-
5.
A condensation of data was repeated 3 times in order to identify the general meaning of the themes explored in order to identify key elements of the perception and use of the technology.
-
6.
A new, final code tree was developed (Textbox 1).
-
7.
Data were presented in themes and findings (see Textbox 2)


3 Findings
Textboxes 1 and 2 show the main themes with the respective subthemes and the key findings from the study.
Baseline demographic characteristics (Table 3) show a majority of men participated in the study. Besides civil status and education level, the ABI patients at home and mentors shared approximately the same baseline characteristics as regards age, home care and children. No differences in the perception of the technology were found based on sex, age, civil status, number of children, education or extent of home care assistance.
Half of the ABI patients at home (n = 4) ended the intervention after one session, and the other half (n = 4) after 3 sessions. One ABI patient at home had no sessions, having stated during the introduction that he had visited ARC previously and did not want to take part in ARC through OriHime, which was the criteria for participating in the interview.
3.1 OriHime as a technology
The ABI patients at home and the mentors had a positive attitude about the technology. They found it easy and practical to use as a communication tool.
It was exciting to see that it [the technology] works so easily. I think it had some very easy methods (C7, male)
As the observational notes show, most of the ABI patients at home were able to use OriHime’s functions, while others needed some assistance from the social workers. In some cases, we observed that the sequelae from ABI, such as hand paresis or sight problems, were too severe and prevented the ABI patient at home from holding the tablet or using its functions.
I cannot see everything. I have to watch one thing at the time, if it has to be this way (C3, female)
We observed during the intervention that the mentors were aware of the lack of human features when using OriHime. After a session, they stated that they missed the social interaction where they could ‘read’ the person as they would normally do when a new member came to the ARC. It was difficult for the mentors to interact with a robot and not a real person; however, they got used to it.
You had to get used to [the OriHime] in the beginning, because you had to get used to the other person not being present, and I think that was the hardest part. The easiest thing was just to do it, as if it were a person anyway, and this is also the way I do it [the intervention] now. (M4, male)
Some of the ABI patients at home perceived the technology as familiar, since they were talking to a tablet, which was similar to talking to a computer, but one did not accept the technology and preferred to talk with a real person.
It was almost like talking to the computer. We are getting used to this technology. I think it was fun. As long as it keeps evolving. (C1, male)
I really do not know because a human and a robot are two separate things. I would prefer to speak with a human rather than a robot. I found it a little strange. (C3, female)
During the intervention, we encountered some technical difficulties that negatively affected OriHime’s functionalities and the communication channels. The difficulties were caused mainly by an unstable internet connection, which affected the sound and video quality and thus made it difficult for the ABI patients at home and mentors to see or hear each other; this caused confusion regarding whether the ABI patient at home behind OriHime was present or not.
I think that the sound quality is bad, it should have been better. (C8, male)
No, I think [the mentor] got confused because [OriHime] was not working. (C4, male)
3.2 Interpersonal communication
The ABI patient at home and mentors appreciated the different communications options offered by OriHime, as OriHime could create a connection with the between them.
Well, I think that was really good because it was like having a bit more connection with the person, if you didn’t just tell them [about ARC], but he asked questions too. (M1, male)
Most of the ABI patients at home used verbal communication, but OriHime’s functions also enabled them to use nonverbal communication as well, so they were not compelled to speak if they did not wish to.
It was fine you could turn off [the microphone] (C2, female)
For the mentors, it was important to get feedback from OriHime, so that they could understand what the ABI patients at home were saying.
The most common functions that the ABI patients at home used from the iPad during the intervention was to move OriHimes head to look around ARC as well as facing the mentor they were interacting with, waving OriHime’s arms to say ‘hi’ or ‘goodbye,’ to turn on/off the microphone when they wanted talk or not and the built-in function ‘clap’ as a reaction to acknowledge the mentor when the guided tour at ARC or activity had ended.
The last time I spoke with that person it went really well, and the movements [i.e., OriHime’s functions] also worked, just that you get a response is positive. (M2, male)
3.3 Community of practice
The majority of the ABI patients at home stated that the intervention with OriHime was meaningful to them, and all ABI patients at home agreed that it was pleasant to experience ARC before taking the decision to visit the club themselves. This was mainly because they obtained familiarity with what the community had to offer as well as the club atmosphere.
Yes, now that I know what [the ARC] is like visually, then you can get to know how it would be to be there. It actually made me calmer. It’s a good place [to go] when I’m ready.
(C2, female)
The mentors also perceived OriHime as meaningful to use so that they could show ARC to the ABI patients at home and help them take that final step of actually visiting ARC.
Yes, the thing that makes sense is that you can take the final step to come in here [to the club]. That they can see, that there is nothing to be afraid of. (M2, male)
Mentors explained their community of practice at ARC as important element for their social interaction with others having the same symptoms, enabling them to learn from each other about how to cope with their brain injury. We observed that this information had been transmitted during the intervention to the ABI patients at home.
[ABI patients at home] can come here and talk to equals. I think it is important for the person. It’s about being able to overcome it, and then come here and talk to other people. And we can tell them through OriHime. (M2, male)
They were doing housekeeping chores [at ARC] to start off with, then the mentor came over and told us that he had also had a stroke. It was good to hear that there are things he also suffers from. (C9, male)
Although mentors shared their community of practice through OriHime, they had different opinions as to whether OriHime was capable of giving a full and realistic picture of ARC, since some members altered their behavior when OriHime was present.
I do not think so [You don’t get the full experience of ARC through OriHIme]. You cannot feel the connection we have with each other in here. You can see what happens, but that’s it. There is also a lot of humor in here and you don’t get that through OriHime. It’s not possible. […] In the kitchen, we have a lot of joking around and teasing each other, but we don’t do that when there is something like that on [i.e., OriHime], because it gets a little more unnatural. You cannot avoid it when there is something like that watching you. (M1, male)
Our observational notes, however, indicate that members still made jokes and teased each other while OriHime was present.
During the meetings at the ARC, we encountered a few members who expressed concern about being under surveillance by OriHime since they did not know who was watching. However, we observed that these members did not visit ARC so frequently and were not present during the intervention. In contrast to the ABI patients at home fears of surveillance, the mentors had a more positive attitude toward OriHime, stating that they felt that it was safe to use during the meetings.
3.4 Motivation to participate at ARC
After the intervention, the ABI patients at home stated that they wanted to visit ARC if they felt that the activities and facilities were useful to them. The activities included knitting with one hand, cooking or having a room to rest. Another reason for wanting to visit ARC was to interact with others who had an ABI, since they had a better understanding of each other’s difficulties than others who might not be able to relate to them.
It’s nice that [other ARC members] also have an injury, as many of the things [symptoms] that I have are also something they are dealing with. There is probably someone who has been coming [to ARC] for many years with those [same symptoms]. It’s hard to explain to other people what it’s like [having an ABI], but they [ARC members] may understand it better. It could be good to come to such a place, because when you are with ordinary people like [names a relative] then it doesn’t matter what I say. She will respond that she feels the same way, and that she knows perfectly how things are, and yeah, it’s fine, but sometimes it’s just hard to explain it in words.
(C2, female)
We observed during a session that an ABI patient at home and a mentor shared information about their condition and subsequently agreed to meet at ARC.
ABI challenges prevent participation in activities or social interaction, even when the ABI patients at home expressed an interest in visiting ARC.
My problem is that if there are many [people] there [at ARC], then I think I would run away. I wouldn’t, but I would go and hide somewhere. (C8, male)
The main problems of attending the ARC were related to being with a lot of people and not having enough energy due to other daily activities such as household chores or rehabilitation exercises. One ABI patient at home comments:
My conscience is not ready yet, and I’m afraid that it will accumulate. I’m so scared of that. Then I suddenly cannot manage it [doing the household chores]. It’s my biggest fear. (C2, female)
Of the nine ABI patients at home in the study, one (C5, female) showed an interest in some of the club activities and visited ARC after one session with the intervention.
4 Discussion
4.1 Using OriHime as a technology
Our findings indicate that many of the participants had a positive attitude about the technology and found it easy to use. However, not all ABI patients at home actually used OriHime’s functions, either because they chose not to or because they were physically unable. This could be a barrier to the use of the technology. Our observations showed that their inability to use OriHime was due to their sequelae from ABI. These obstacles are consistent with other studies showing that persons with an ABI often suffer from sequelae conditions [7]. Therefore, the ABI patients at home physical challenges should be taken into account when deploying the technology. In addition, even though we tried to minimize the potential risks of technical difficulties throughout the intervention by performing pilot tests of the technology, we did have to interfere a few times during the intervention due to connectivity difficulties. Also, a few of the ABI patients at home had some starting issues on using the controlling functions to the OriHime from the iPad where we had to interfere, but after some practical experience with the app on the iPad they were capable of using the functions.
The ABI patients at home became accustomed to using the technology and did not feel unusual, probably due to the normality of owning a smart device in Denmark [33].
Some of the mentors, however, stated that they found that talking to OriHime was strange and unnatural, and one mentor said he would prefer to give a guided tour to a physical person rather than via the robot, because he would then be able to see their nonverbal language, such as facial expressions, thus making the social interaction more human-like and easier to decipher. A review of studies in social psychophysics has addressed this problem concerning the use of social robots and avatars [34]. The review argues that future research within the field of social robotics should focus on the challenges of recreating facial expressions, as it is important in human communication and perception, e.g., in judging a person by their appearance to understand the underlying meaning of what is spoken as well as trustworthiness [34]. This lack of feedback in the form of facial expression might explain why some mentors felt that their interaction with OriHime was so awkward.
4.2 Interpersonal communication
Our findings support those of other studies highlighting the value of verbal and nonverbal communication for patients in social psychiatry [16, 22]. This is certainly why mentors expressed the importance of feedback during the intervention. Our study further highlights the value of persons with ABI having the option to choose between verbal and nonverbal communication channels. This option was particularly valuable for some ABI patients at home who did not want to communicate verbally, as they felt their voice was different following the ABI and that this altered voice made them feel uncomfortable speaking to strangers. This issue, consistent with findings from other studies on ABI implications [8, 9], indicates that OriHimes features can be valuable for patients with an ABI because it provides options of communication. As an avatar, OriHimes nonverbal features can add an extra dimension to the communication. This could potentially lead to more substantial social interaction when communicating over distance. Nevertheless, the mentors preferred verbal to nonverbal communication because it provided a better connection with the person communicating through OriHime. Our findings suggest that the differing views of the ABI patients at home and mentors about the use and value of OriHime might raise an ethical concern, since the ABI patients at home could choose to communicate verbally, nonverbally or not at all, while mentors did not have such a choice. Besides that, OriHime also provided the ABI patients at home with a degree of anonymity, while the mentors’ identity was exposed and was without any facial feedback from the ABI patient at home. It was this lack of feedback that could also create a situation of discomfort. This discomfort became visible during one session, when an ABI patient at home was supposed to verbally communicate but was barely active; the result was an awkward situation where the mentor did not know what to say because the ABI patient, safely hidden at home behind OriHime, was not responding.
4.3 Community of practice
One of the requirements for a community of practice is that trust is needed before members of a community will be willing to share their knowledge and experiences [35]. Our findings are contradictory on this point. On the one hand, they suggest that a community of practice was successfully shared through OriHime and that the mentors trusted their experiences to the ABI patients at home and that some users built bonds of trust with the mentors. However, some of the ARC members had a feeling of being under surveillance, and two mentors stated that the social behavior of the members at ARC changed when OriHime was present. Therefore, we might argue that a community of practice was not achieved through OriHime, since some members did not trust the technology or the person behind it. However, our observations at ARC showed that the members who had feelings of being under surveillance were not as active as those who consistently visited ARC. Also, we observed that throughout the intervention, the ARC members were chatting, teasing and interacting socially as they usually did, even when OriHime was present. This would suggest that a period of familiarization is needed so that people feel comfortable with OriHime and will accept it. This is supported by another study showing that experience with a robot is necessary to achieve acceptance by the patient [22].
4.4 Motivation to participate at ARC
During the intervention, the mentors and members shared a community of practice with the ABI patients at home regarding their ABI and how to cope with other daily activities, such as cooking. Most of the ABI patients at home were positive about visiting the ARC in the future, and one who had not yet visited the ARC made an appointment to meet his mentor at ARC during his first session of the intervention. In our view, this indicates that the interaction provided by OriHime had the potential to motivate the ABI patients at home to participate in rehabilitation activities and socializing, especially if they could create a connection to the mentor. This is supported by a study showing that social support has a positive effect on motivation [36]. Another study also indicates that technologies that create social engagement and connect people who have an ABI are valuable, since this patient group otherwise lacked social contact [37]. However, most of the ABI patients at home were not sure about precisely when they wanted to join ARC, stating that fatigue, transport to ARC and other daily activities prevented them from taking the final step. It is therefore debatable whether the interaction with OriHime had a sufficient impact on the ABI patients at home motivation, or whether the distance to ARC and the difficulty of planning the trip due to fatigue were the deciding factors. While the interaction provided by OriHime and the community of practice created by this interaction certainly had a motivational impact, it was not decisive enough to lead the majority of the ABI patients at home to actually visit ARC because their ABI sequelae apparently had a bigger impact on their decision to refrain from visiting the ARC. OriHime perhaps should therefore be used in conjunction with other more tailored strategies in order to create the optimum benefits. For example, OriHime could be combined with a visit to ARC with their affiliate social worker, or stronger relations of trust could be initially created with the same mentor over a longer period as a prelude to visiting ARC. The benefits of such tailored strategies are highlighted by a study showing that because adults with an ABI are a heterogeneous group, interventions need to be tailored to the individual and their specific challenges [38].
‘C5’ visited ARC after a single session. During the intervention, she became interested in one activity in particular: learning to knit with one hand. However, it is unclear whether it was OriHime that helped C5 to decide to visit ARC by showing her the community of practice, or whether she was predisposed to visit ARC, regardless of the information she acquired. Prior to the intervention, C5 had stated that she was considering visiting ARC in the following week. Later in the interview, however, she said that she was still unsure whether or not she should visit ARC. We know from other studies that the cognitive challenges experienced by persons with an ABI can affect the time it takes to plan and then, e.g., visit a new place [8]. This could explain why C5 needed 6 weeks from the start of the intervention before she finally decided to visit the ARC.
4.5 Limitations
Yin has argued that a multiple case design is preferred over the single case design because it makes the analytics more substantial [23]. Ours was a single case study. We sought to explore whether OriHime could work within a single rehabilitation venue as a prelude to undertaking a larger scale study. Our reasoning was that, to our knowledge, no studies have yet explored the opportunities of using a telepresence avatar robot for patients with an ABI. If our case study were to be expanded to multiple municipalities and rehabilitation venues, our findings on the intervention with OriHime would be more robust and constitute a more solid basis for generalization [39].
The recruitment of the ABI patients at home in our study was carried out by their affiliated social worker. We worked on the assumption that we could trust the social workers’ professional knowledge about this patient group. However, we encountered a semantic issue, due to our inclusion criterion of ‘mild-to-moderate brain injury’ because this particular criterion could be interpreted differently. This potential ambiguity might have impacted the selection and total number of participants in the study because the social workers could have been unsure of what constitutes ‘mild to moderate.’ For the same reason, it was also possible that some of the ABI patients at home might not have been appropriate for the patient group we wanted to recruit, having either too little or severe ABI symptoms. During the introduction meeting with the ABI patients at home, we also evaluated their suitability for our study, but as we have had no experience with ABI patients ourselves, some degree of bias might still have occurred.
When conducting ethnographic field work, the researcher risks getting so involved that their very presence will affect the context, or the researcher can become emotionally attached to the subject and fail to be objective [24].
Our study could fall into this category because the participants were engaging with the investigating authors, and the participants asked the authors about what to tell or talk about during the intervention. However, to the best of our abilities, we tried not to influence the context, and instead of telling the mentors and the ABI patients at home what to say and do, we attempted to act as facilitators, allowing the mentors and ABI patients at home to improvise and discuss how they would normally do during the intervention.
5 Conclusion
The social robot OriHime showed itself to be a useful communication tool for citizens with ABI in attracting them to and experiencing a rehabilitation center. The use of the OriHime resulted in creating a community of practice between the ABI patients at home and mentors of the rehabilitation center. The ABI patients at home became more motivated to participate in social and rehabilitation activities at the center.
Future research is needed in order to study the long-term effects of using the social robot OriHime for patients with an ABI.
References
Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung Y-C, Punchak M et al (2018) Estimating the global incidence of traumatic brain injury, pp 1–18. http://www.ncbi.nlm.nih.gov/pubmed/29701556
Feigin VL, Norrving B, Mensah GA (2017) Semin global burden of stroke. Neurology 38(2):208–211
Proctor CJ, Best LA (2019) Social and psychological influences on satisfaction with life after brain injury. Disabil Health J 12:1–7. https://doi.org/10.1016/j.dhjo.2019.01.001
Bhogal SK, Teasell R, Foley N, Speechley MJ (2005) Heterocyclics and selective serotonin reuptake inhibitors in the treatment and prevention of poststroke depression. Am Geriatr Soc 53(6):1051–1057
Teasdale TW, Engberg AW (2005) Subjective well-being and quality of life following traumatic brain injury in adults: a long-term population-based follow-up. Brain Inj 19(12):1041–1048
WHO (2012) Neurological disorders: public health challenges. WHO. World Health Organization [cited 2019 May 18]. https://www.who.int/mental_health/neurology/neurodiso/en/
Strandberg T (2009) Adults with acquired traumatic brain injury: experiences of a changeover process and consequences in everyday life. Soc Work Health Care 48(3):276–297
Paterson J, Stewart J (2012) Adults with acquired brain injury: perceptions of their social world. Rehabil Nurs 27(1):13–18
Secrest JA, Thomas S (1999) Continuity and discontinuity: the quality of life. Rehabil Nurs J 24(6):240–246
Teasdale TW, Engberg AW (2001) Suicide after traumatic brain injury: a population study. J Neurol Neurosurg Psychiatry 71(4):436–440
McCabe P, Lippert C, Weiser M, Hilditch M, Hartridge C, Villamere J (2007) Community reintegration following acquired brain injury. Brain Inj 21(2):231–257
Wolf TJ, Chuh A, Floyd T, McInnis K, Williams E (2014) Effectiveness of occupation-based interventions to improve areas of occupation and social participation after stroke: an evidence-based review. Am J Occup Ther 69(1):6901180060p1. https://doi.org/10.5014/ajot.2015.012195
Häggström A, Lund ML (2008) The complexity of participation in daily life: a qualitative study of the experiences of persons with acquired brain injury. J Rehabil Med 40(2):89–95
Turner B, Fleming J, Cornwell P, Worrall L, Ownsworth T, Haines T et al (2007) A qualitative study of the transition from hospital to home for individuals with acquired brain injury and their family caregivers. Brain Inj 21(11):1119–1130
Chen S-C, Jones C, Moyle W (2018) Social robots for depression in older adults: a systematic review. J Nurs Scholarsh 50(6):612–622. https://doi.org/10.1111/jnu.12423
Pu L, Moyle W, Jones C, Todorovic M (2018) The effectiveness of social robots for older adults: a systematic review and meta-analysis of randomized controlled studies. Gerontologist 59(1):E37–E51
Papadopoulos I, Koulouglioti C (2018) The influence of culture on attitudes towards humanoid and animal-like robots: an integrative review. J Nurs Scholarsh 50(6):653–665
Góngora Alonso S, Hamrioui S, de la Torre Díez I, Motta Cruz E, López-Coronado M, Franco M (2018) Social robots for people with aging and dementia: a systematic review of literature. Telemed e-Health 00(00):10–12
Shishehgar M, Kerr D, Blake J (2018) A systematic review of research into how robotic technology can help older people. Smart Heal 1:1. https://doi.org/10.1016/j.smhl.2018.03.002
Moyle W, Bramble M, Jones CJ, Murfield JE (2017) “She had a smile on her face as wide as the great australian bite”: a qualitative examination of family perceptions of a therapeutic robot and a plush toy. Gerontologist 59(1):177–185
Strandbech JD (2018) Humanoid robots for health and welfare: on humanoid robots as a welfare technology used in interaction with persons with dementia. Aalborg Universitetsforlag. 251 s. (Aalborg Universitet. Det Humanistiske Fakultet. Ph.D.-Serien) https://doi.org/10.5278/vbn.phd.hum.00092
Moyle W, Arnautovska U, Ownsworth T, Jones C (2017) Potential of telepresence robots to enhance social connectedness in older adults with dementia: an integrative review of feasibility. Int Psychogeriatr 29(12):1951–1964
Yin RK (2018) Case study research and applications—design and methods. In: Oaks T, 6th edn, COSMOS Corporation, United States
Hammersley M, Atkinson P. Ethnology; Principles in Practice [Internet]. 2007 [cited 2019 Feb 20]. 14–17 p. Available from: http://web.b.ebscohost.com.zorac.aub.aau.dk/ehost/ebookviewer/ebook/bmxlYmtfXzE5NzI1M19fQU41?sid=0f249291-ca58-4a39-9959-c88e07dbac34@sessionmgr120&vid=0&format=EK&lpid=ac-6&rid=0
InterSoft Consulting (2018) General data protection regulation (GDPR)—final text neatly arranged. EU [cited 2019 Jun 4]. https://gdpr-info.eu/?fbclid=IwAR3Xk0NPOSqNSY2_E50X13XTHXhwjkfnKElapwJEQ3LFjWHUg2R6fjRck0A
Datatilsynet.dk. Tv-overvågning (2019) [cited 2019 Jun 4]. https://www.datatilsynet.dk/emner/overvaagning-og-sporing/tv-overvaagning/
ARK. ARK Aalborg er en ArbejdsRehabiliteringsKlub i Aalborg. [cited 2019 May 18]. https://handicaptilbuddene.aalborg.dk/fagcentre/fagcenter-for-erhvervet-hjerneskade-og-fysisk-handicap/ark-aalborg
OryLab. OriHime by Ory Laboratory. [cited 2019 Jun 4]. http://ces15.orylab.com/
Wenger E, White N, Smith JD (2009) Digital habitats: stewarding technology for communities. CPsquare, Portland
Wenger-Trayner E and B. Communities of practice—a brief introduction. www.wenger-trayner.com. 2015 [cited 2019 Apr 10], pp 1–8. https://wenger-trayner.com/wp-content/uploads/2015/04/07-Brief-introduction-to-communities-of-practice.pdf
Tanggaard L (2010) Kvalitative metoder og tilgange: en grundbog. Hans Reitzel. [cited 2019 May 18], 560 pp. https://www.saxo.com/dk/kvalitative-metoder_svend-brinkmann_indbundet_9788741259048?dfw_tracker=13098-21157778&gclid=Cj0KCQjw2v7mBRC1ARIsAAiw3485zUva2aV7EZwMIw6G-iZeqQD0s5aKk_KWacBXK-GIpqHmM-5SCEQaAswLEALw_wcB
Kvale S, Brinkmann S (2009) Interview: introduktion til et håndværk. Hans Reitzel [cited 2019 May 18]. https://bibliotek.dk/da/work/810015-katalog%3A009100625
Statistik D, Helle A, Holm H, Statistik D, Statistik D (1996) Vores tro digitale følgesvend fylder 20 år. 2016 [cited 2019 May 30], pp 8–10. https://www.dst.dk/da/Statistik/bagtal/2016/2016-08-30-vores-tro-digitale-foelgesvend-fylder-20-aar
Jack rachael, Schyns PG. Toward a Social Psychophysics of Face Communication. Ssrn. 2017 (2017)
Roberts J (2006) Limits to communities of practice. J Manag Stud 43(3):623–639
Kusec A, Velikonja D, DeMatteo C, Harris JE. Motivation in rehabilitation and acquired brain injury: can theory help us understand it? Disability and rehabilitation, pp 1–7. https://www.tandfonline.com/action/journalInformation?journalCode=idre20
Jamieson M, Jack R, O’Neill B, Cullen B, Lennon M, Brewster S et al (2019) Technology to encourage meaningful activities following brain injury. Disabil Rehabil Assist Technol. https://www.tandfonline.com/action/journalInformation?journalCode=iidt20
Brett CE, Sykes C, Pires-Yfantouda R (2017) Interventions to increase engagement with rehabilitation in adults with acquired brain injury: a systematic review. Neuropsychol Rehabil 27:959–982
Flyvbjerg B (2006) Five misunderstandings about case-study research. Qual Inq 12(2):219–245
Acknowledgments
The investigating authors wish to thank the ABI patients at home, mentors and members of the ARC who participated in this study, as well as the staff at ARC and the social workers who helped us in the planning of the study and recruiting the participants. We also wish to thank Lars Nøhr, Chief Consultant of Aalborg Municipality and Kristian Kjeldsgaard Liltorp, Assistant Director of ARC. Thanks to the Laboratory for Welfare Technology, Telehealth and Telerehabilitation, Department of Health Science and Technology at Aalborg University, Denmark, for providing telecommunication facilities and supervision through the study. And finally, we thank OryLab for providing the OriHime (named after the tale of princess OriHime) robot used in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The investigating authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix




Rights and permissions
About this article

Cite this article
Vikkelsø, S., Hoang, TH., Carrara, F. et al. The telepresence avatar robot OriHime as a communication tool for adults with acquired brain injury: an ethnographic case study. Intel Serv Robotics 13, 521–537 (2020). https://doi.org/10.1007/s11370-020-00335-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11370-020-00335-6