
Abstract
Melanoma is the most fatal type of skin cancer. Non-invasive melanoma detection is crucial for preliminary screening and early diagnosis. Among various image based techniques, hyperspectral imaging is a tool with great potential for melanoma detection since it provides highly detailed spectral information beyond the human vision capability. However, so far no hyperspectral image dataset has been published, although some pilot methods have been studied. In this paper, we introduce a hyperspectral dermoscopy image dataset for melanoma detection. This dataset consists of 330 hyperspectral images with 16 spectral bands each in the visible wavelength, containing images of melanoma, dysplastic nevus, and other types, all histopathologically validated. To build a baseline for melanoma detection, we evaluate several classification methods on the dataset.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Skin cancer accounts for the most common among all newly diagnosed cancers in Australia and in USA [1, 2]. The Cancer Council Australia estimated that two in three Australians will be diagnosed with skin cancer by the time they are 70 years old [1]. Skin cancer can be classified as melanoma and non-melanoma. Melanoma is the most deadly type of all skin cancers [1], although it is not the most prevalent type.
An early screening of melanoma can greatly increase the chance of cure. During the diagnosis process, dermoscopy has been widely used to provide a detailed and magnified view of skin. However, it is still a challenging problem to overcome the subjectivity of dermatologists in differentiating melanoma from benign pigmented lesions, as melanoma shows great similarity with nevus, solar lentigo etc. Although experienced clinicians can make initial screening, histology of biopsy is the only confident way of final diagnosis. This, however, is often restricted by the available resources. Therefore, an early computer aided screening of skin cancer is of high interest to help dermatologists to make the diagnosis objective and to increase the speed and accuracy of pre-diagnosis.
Existing computer aided systems for melanoma detection are mainly developed based on clinicians’ visual assessment methods, such as the ABCD (asymmetry, border, color, dimension) rules [3]. In many cases, the early decision also combines existence of subtle features, such as irregular streaks [4], pigment network [5], and blue-white veil [6] etc. In more recent, deep learning based methods have been proposed so as to avoid development of hand crafted features [7,8,9,10], which has demonstrated state-of-the-art detection performance.
Traditional imaging systems normally capture color or grayscale images in the visible wavelengths. They do not have the capability of detecting fine changes of skins with respect to the light wavelength change. Hyperspectral imaging is a technique that combines both spatial information provided by conventional imaging system and spectral information of imaging spectroscopy. Comparing with traditional imaging system, besides characterising the spatial distribution of pigmented skin lesion, hyperspectral imaging provides the potential of measuring concentration of melanin and hemoglobin molecular by analysing reflectance spectra. Therefore, this technology gradually attracts the attention in skin related medical imaging [13], such as burn characterization [14] and gunshot assessment [15]. A melanoma mouse model was build on hyperspectral imaging [18], which shows the potential of diagnostic improvements. Hyperspectral melanoma images were analysed by Zherdeva et al. [16], with band selection method proposed to select the most informative wavelength for cancer detection [17]. Nagaoka et al. proposed a melanoma discrimination index method using hyperspectral data in the visible to near infrared wavelength range [19], which achieved high sensitivity on a small dataset.
Most existing hyperspectral imaging systems are expensive and not portable. Some of them use line-scan hyperspectral cameras, which are slow in image acquisition. These have generated a lot of hurdles in clinical operation and producing a public hyperspectral skin image dataset for research purpose. In this paper, we introduce a hyperspectral dermoscopy imaging dataset captured using a portable real-time imaging system. The dataset contains 330 dermoscopy images which are all histology verified, including 85 melanomas, 175 dysplastic nevi and 70 other pigmented lesions (solar lentigo, IEC, nevi and Seborrheic Keratosis). Each image has 16 bands, covering the wavelength from 465 nm to 630 nm. We also provide bounding boxes on melanocytic human skin lesions to support the training and evaluation of melanoma detection methods.
The rest of the paper is organised as follows. We present the dataset and its statistics in Sect. 2. The baseline detection approach and experimental results are given in Sect. 3. Finally, conclusions are drawn in Sect. 4.
2 Hyperspectral Dermoscopy Dataset
This section introduces the imaging system and how to calibration of captured images. It also provides basic data analysis on different skin images.

Spectral responses at a pixel on original and calibrated images.
2.1 Imaging System and Calibration
The main hardware of the image system includes a portable device and an Ximea MQ022HG-IM-SM4X4-VIS camera. The portable devices consists of a Raspberry PI, a 7 in. touch screen, an 8G Raspberry PI compatible MicroSD card, and a set of nickel–metal hydride batteries, all sealed in a box. Together with the portable device, the camera can be put on top of dermatoscope to capture magnified image of skin lesion. The dermatoscope provides visible light from LED, with which the Ximea camera is capable of capturing hyperspectral images of 16 bands from 465 nm to 630 nm. Each band image is constituted of approximately \(512\times 272\) pixels. The Ximea camera is only 32 grams in weight and can capture hyperspectral images at up to 170 cubes per second. The camera is operated using a lab developed software which allows image capture and management.
Each captured image consists of \(1024\times 2048\) pixels arranged in \(256\times 512\) blocks of spatial information. Each block contains 4 rows and 4 columns of grayscale values, corresponding to spectral information from 16 wavelength-indexed bands. Therefore, each image can be converted into a \(256\times 512 \times 16\) data cube, which is later processed with dark and white calibration as well as camera based spectral correction. In dark calibration step, we deducted a dark image (captured with lens cap on) from the captured image. For white calibration, we normalised the image with the mean of the selected region from a white calibration board. Finally, we performed spectral calibration, which multiplies the image with a correction matrix corresponding to the sensitivity function associated with the CMOS sensor of the camera. The three preprocessing steps can be formulated as:
where \(I_o\) is the original data cube converted from the raw image, \(I_b\) is the black reference data cube, \(I_w\) is the white reference data cube which is obtained by capturing image of the white calibration board under the dermatoscope, and C is a \(16\times 16\) correction matrix which is related to the camera. Figure 1 shows the comparison of a sample spectral response after different operations of calibration.

Band images of two samples.
2.2 Data Collection and Basic Spectral Analysis
The collection of this hyperspectral dermoscopy image dataset is a joint collaboration between our research team and a local Skin Cancer Clinic. Before the data collection, we went through an ethics approval, so only the clinic staff can get in contact with the patients and get their consent. All patient’s privacy information are protected without being released to people other than the clinic. The clinic doctor helped to collect the images with the developed portable hyperspectral imaging device and a dermatoscope of 10 times of magnification. All images were captured before biopsy which were later taken to pathologists for final diagnosis. Then, all the images were labeled according to diagnosis reports. The first stage data collection started from 6th January, 2017 and ended on 18th February, 2018.
In total 330 hyperspectral dermoscopy images with good quality were selected to build the dataset. These include 80 melanoma images, 180 dysplastic nevus images and 70 other images for solar lentigo, IEC, nevi and Seborrheic Keratosis. We manually labelled the legion regions using bounding boxes. Two dysplastic nevi and melanoma data samples with bounding boxes are illustrated in Fig. 2. We also show in Fig. 3 some sample images of each lesion class in the dataset, including melanoma, solar lentigo, IEC, dysplastic nevi, nevi and Seborrheic Keratosis.

Sample images in the dataset (the 11th band). First row from left to right: melanoma, solar lentigo and IEC. Second row from left to right: dysplastic nevi, nevi and Seborrheic Keratosis.
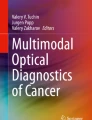
To compare the spectral responses of typical targets in the captured image, we plot sample responses of melanoma (green plus sign), dysplastic nevus (red dots), hair (blue stars) and normal skin (cyan triangles) in Fig. 4. Among all the spectra, normal skin shows the highest intensities, as it is inherently lighter than other lesions. Intensities of hair, dysplastic nevus and melanoma are roughly in the same level of intensity, although hair spectrum is slightly less steady than the other two. Moreover, we notice that cancer/non-cancer spectra are close to each other, which implies effective spectral-spatial analysis methods shall be developed to distinguish them.
3 Baseline Method
To validate the feasibility of the proposed dataset, we developed a sparse coding method [20, 21] to classify the images in the hyperspectral dataset, and compared the results with those obtained on RGB images of the same scene. The RGB images were generated from the hyperspectral images by sampling band images at 630 nm, 546 nm and 465 nm, which roughly correspond to the centers of the red (610–700 nm), green (500–570 nm), and blue (450–500 nm) wavelength ranges [22].
The baseline method has three main steps. First, we randomly sampled spectral responses from the labelled bounding boxes in the training images. The bounded image is evenly divided into grids, with half of the points in each grid used to produce a sparse dictionary. Then sparse codes were calculated on each image followed by max pooling to convert the image into a vector. Finally, the vectorised images were used to train a multi-class SVM classifier. Please note that this baseline method is purely based on spectral analysis. In RGB image classification, we used the same SVM classifier, but adopted local binary patterns [23] for feature extraction. In the experiments, we randomly sampled 60 images from each class as training samples, and used the rest images as the testing samples. The random split of training and testing sets were done for five times with the mean and standard deviation of the results reported.

Different regions and their spectral responses. (a) Melanoma. (b) Nevus and normal skin. (c) Hair. (d) Corresponding spectral responses. (Color figure online)
3.1 Experimental Results
We use sensitivity (ratio between true positive and all positive cases) and specificity (ratio between true negative and all negative cases) to evaluate the performance of our sparse coding method. Since melanoma is considered as the true case, all correctly predicted melanoma samples are true positive, while all wrongly predicted other cases are false negative. In the classification, we tried both three-class (melanoma VS dysplastic nevi VS Other type) and two-class (melanoma VS dysplastic Nevi) settings.
The result comparison is given in Table 1. It can be seen that the performance of classification based on hyperspectral images is much better than that from RGB images. This proves that spectral information is useful for melanoma detection. Moreover, all 2-class classification results are better than 3-class classification. Standard deviations of all 3-class classification results are high, due to the large variation and the small size of the third class, namely the other type. We also tested the case when the size of the lesion is added as an additional feature for hyperspectral image classification. The results show that the performance is improved, which implies that size is an important feature for differentiating melanoma from the other types.
4 Conclusion
We have presented a hyperspectral imaging dataset of 330 histology verified skin lesion images. The images in the dataset are calibrated and with lesion regions provided using bounding boxes. This dataset provides a foundation for further research on hyperspectral imaging techniques and its usefulness in early screening of skin cancers using image based approaches, namely wavelength analysis. The experimental results on a baseline approach show that pure spectral analysis is not sufficient to reliably detect melanoma. More effective spectral-spatial data analysis approach and advanced classification approaches are yet to be developed. In the future, we will also continue to explore and collaborate with skin cancer clinics for more data collection.
References
Cancer Council Australia. https://www.cancer.org.au/about-cancer/types-of-cancer/skin-cancer.html. Accessed 2 May 2018
America Cancer Society. https://www.cancer.org/cancer/skin-cancer.html. Accessed 30 July 2018
Rastgoo, M., Garcia, R., Morel, O., Marzani, F.: Automatic differentiation of melanoma from dysplastic nevi. Comput. Med. Imaging Graph. 43, 44–52 (2015)
Sadeghi, M., Lee, T.K., McLean, D., Lui, H., Atkins, M.S.: Detection and analysis of irregular streaks in dermoscopic images of skin lesions. IEEE Trans. Med. Imaging 32(5), 849–861 (2013)
Sadeghi, M., Razmara, M., Lee, T.K., Atkins, M.S.: A novel method for detection of pigment network in dermoscopic images using graphs. Comput. Med. Imaging Graph. 35(2), 137–143 (2011)
Madooei, A., Drew, M.S., Sadeghi, M., Atkins, M.S.: Automatic detection of blue-white veil by discrete colour matching in dermoscopy images. In: Mori, K., Sakuma, I., Sato, Y., Barillot, C., Navab, N. (eds.) MICCAI 2013. LNCS, vol. 8151, pp. 453–460. Springer, Heidelberg (2013). https://doi.org/10.1007/978-3-642-40760-4_57
Codella, N., Cai, J., Abedini, M., Garnavi, R., Halpern, A., Smith, J.R.: Deep learning, sparse coding, and SVM for melanoma recognition in dermoscopy images. In: Zhou, L., Wang, L., Wang, Q., Shi, Y. (eds.) MLMI 2015. LNCS, vol. 9352, pp. 118–126. Springer, Cham (2015). https://doi.org/10.1007/978-3-319-24888-2_15
Yu, L., Chen, H., Dou, Q., Qin, J., Heng, P.A.: Automated melanoma recognition in dermoscopy images via very deep residual networks. IEEE Trans. Med. Imaging 36(4), 994–1004 (2017)
Xie, F., Fan, H., Li, Y., Jiang, Z., Meng, R., Bovik, A.: Melanoma classification on dermoscopy images using a neural network ensemble model. IEEE Trans. Med. Imaging 36(3), 849–858 (2017)
Esteva, A., et al.: Dermatologist-level classification of skin cancer with deep neural networks. Nature 542(7639), 115 (2017)
Chang, I.: Hyperspectral Imaging: Techniques for Spectral Detection and Classification. Springer, New York (2003). https://doi.org/10.1007/978-1-4419-9170-6
Wei, X., Liu, F., Qiu, Z., Shao, Y., He, Y.: Ripeness classification of astringent persimmon using hyperspectral imaging technique. Food Bioprocess Technol. 7(5), 1371–1380 (2014)
Lu, G., Fei, B.: Medical hyperspectral imaging: a review. J. Biomed. Opt. 19(1), 010901 (2014)
Calin, M.A., Parasca, S.V., Savastru, R., Manea, D.: Characterization of burns using hyperspectral imaging technique-a preliminary study. Burns 41(1), 118–124 (2015)
Kersh, K.L., Childers, J.M., Justice, D., Karim, G.: Detection of gunshot residue on dark-colored clothing prior to chemical analysis. J. Forensic Sci. 59(3), 754–762 (2014)
Zherdeva, L.A., Bratchenko, I.A., Myakinin, O.O., Moryatov, A.A., Kozlov, S.V., Zakharov, V.P.: In vivo hyperspectral imaging and differentiation of skin cancer. In: Optics in Health Care and Biomedical Optics VII, vol. 10024, p. 100244G. International Society for Optics and Photonics (2016)
Quinzan, I., Sotoca, J.M., Latorre-Carmona, P., Pla, F., Garcia-Sevilla, P., Boldo, E.: Band selection in spectral imaging for non-invasive melanoma diagnosis. Biomed. Opt. Express 4(4), 514–519 (2013)
Tsapras, A., et al.: Hyperspectral imaging and spectral classification for assisting in vivo diagnosis of melanoma precursors: preliminary results obtained from mice. In: IEEE International Conference on Imaging Systems and Techniques, pp. 379–383 (2016)
Nagaoka, T., Nakamura, A., Kiyohara, Y., Sota, T.: Melanoma screening system using hyperspectral imager attached to imaging fiberscope. In: Annual International Conference of the IEEE Engineering in Medicine and Biology Society, pp. 3728–3731 (2012)
Cai, D., Bao, H., He, X.: Sparse concept coding for visual analysis. In: IEEE Conference on Computer Vision and Pattern Recognition, pp. 2905–2910 (2011)
Yang, J., Yu, K., Gong, Y., Huang, T.: Linear spatial pyramid matching using sparse coding for image classification. In: IEEE Conference on Computer Vision and Pattern Recognition, pp. 1794–1801 (2009)
Su, H., Du, Q., Du, P.: Hyperspectral image visualization using band selection. IEEE J. Sel. Top. Appl. Earth Obs. Remote. Sens. 7(6), 2647–2658 (2014)
Guo, Z., Zhang, L., Zhang, D.: A completed modeling of local binary pattern operator for texture classification. IEEE Trans. Image Process. 19(6), 1657–1663 (2010)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Switzerland AG
About this paper

Cite this paper
Gu, Y., Partridge, YP., Zhou, J. (2018). A Hyperspectral Dermoscopy Dataset for Melanoma Detection. In: Stoyanov, D., et al. OR 2.0 Context-Aware Operating Theaters, Computer Assisted Robotic Endoscopy, Clinical Image-Based Procedures, and Skin Image Analysis. CARE CLIP OR 2.0 ISIC 2018 2018 2018 2018. Lecture Notes in Computer Science(), vol 11041. Springer, Cham. https://doi.org/10.1007/978-3-030-01201-4_29
Download citation
DOI: https://doi.org/10.1007/978-3-030-01201-4_29
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-01200-7
Online ISBN: 978-3-030-01201-4
eBook Packages: Computer ScienceComputer Science (R0)