
Abstract
Obsessive-Compulsive Disorder (OCD) is a chronic disease stated by United Nations as one of the 10 most disabling illnesses and key factor in decreased quality of life. It affects millions of people around the world, reaching a population equivalent of countries like Germany or Mexico. One of most used and effective treatment is Cognitive-Behavioral Therapy (CBT) but, its failure rate can be as high as 30%. Games have been greatly incorporated to everyday lives of millions of people, and because of that, are becoming a useful tool to help in healthcare - becoming what is called Games for Health (GfH). This literature review seeks to research academic papers that demonstrate the use of games to treat OCD - as games standalone or in conjunction with CBT. The main objectives of this literature review are to summarize the previous published works and to gather base knowledge in the area for future research developments.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
In recent years, the development of digital technologies has made game creating easier. At the same time, the health area has been using these technologies to make games specially tailored to fit several areas of the healthcare system and several researches have shown the relevance of digital games, either as a support tool in the diagnostic process or during the treatment of various pathologies. Usually, these games are called Games for Health (GfH), they are health-related computer games, or similar computer applications that use software tailored to computer game development [1] and can have their focus on treatment, diagnosis, rehabilitation [2, 3]; on developing applications that implement games [4]; or on education, integration and socialization [5, 6]. When it comes to adapting new gaming technology for specialized health contexts, the scenario is full of interesting perspectives [7], a growing body of research indicates that GfH provide measurable health benefits [1].
Several kinds of games have been designed to support the training of health professionals, providing an environment for them to practice skills before embracing real situations. There is also a substantial variety in types of diseases considered by these training games, such as malaria [8], metabolic syndrome, diabetes mellitus, dyslipidemia, obesity [2], or diagnosis of breast problems [9]. However, all those efforts using technology to improve diagnosis can only succeed properly if the health system could be strong and fluid instead of a barrier [3].
Another relation between games and health is supporting treatments, for example, neurodevelopment treatment techniques for persons with traumatic brain injury [10]; a contrast-based game for treating both adults and children with amblyopia [11]. Games can also be part of preventive treatment, through an educational perspective, allowing the number of emergency clinical utilization to be reduced the longer patients spend playing and learning about their own self-care needs [12, 13].
Besides using games on health diagnosis or treatment, there is another possibility: Gamification, which means the “use of gameplay mechanics for non-game applications” [14], for example, adding game elements to standard computerized working memory (WM) to observe if it would enhance motivation and training performance of children with Attention Deficit Hyperactivity Disorder - ADHD [15].
The use of digital games specifically for treatments of ‘mental health’ began in the early 1990s with the use of high popular entertainment games such as Mario Bros series [16]; technology advances have facilitated, decades later, the development of specialized games, allowing researchers to apply games that can provide specific functions for treatments in psychotherapy [17, 18]; or even innovating through Patents of Methods to support psychological and emotional disorders [19]. Wilkinson [20] has observed a greater number of experiences through the offline games and highlights the potential of the online game in therapy because of the characteristics of the online game world which can both motivate, challenge and be governed by rules tailored by specific needs. Finally, one possible way to categorize the use of games on mental health context is games for prevention and games for health support [21]. Therefore, it is known that the use of smartphone applications increases the quality and results of behavioral health care [22].
2 Obsessive-Compulsive Disorder - OCD
Obsessive-Compulsive Disorder (OCD) is a chronic disease with periods of remission and relapse [23]. According to Veale and Roberts [24], OCD is the fourth most common mental disorder after depression, alcohol/substance misuse, and social phobia, and its global prevalence is estimated between 1.2 to 3% of the general population [25]. It occurs all over the world, and tends to be about one-and-a-half to two times more likely for women to meet criteria for OCD in their lifetime than men [26]. The first manifestations of OCD often appear between ages 8 and 11, with an increase in OCD diagnosis during puberty and again in early adulthood [25]. Also, persons with OCD were likely to have major depression or any other anxiety disorder as a comorbid condition [27]. The following, from the American Psychiatric Association, is the definition considered in this review [28]:
“OCD is characterized by the presence of obsessions and/or compulsions. Obsessions are recurrent and persistent thoughts, urges, or images that are experienced as intrusive and unwanted, whereas compulsions are repetitive behaviors or mental acts that an individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly. Some other obsessive-compulsive and related disorders are also characterized by preoccupations and by repetitive behaviors or mental acts in response to the preoccupations. Other obsessive-compulsive and related disorders are characterized primarily by recurrent body-focused repetitive behaviors (e.g., hair pulling, skin picking) and repeated attempts to decrease or stop the behaviors”.
(AMERICAN PSYCHIATRIC ASSOCIATION, 2013).
According to Bream [26], the individual with OCD, when in contact with certain triggers, have recurrent, specific thoughts, images, impulses, or doubts that remain against their will, and create awareness of the potential for danger which the person can cause or prevent, and these are called obsessions. As a result of them, the person performs actions that are also specific, which act as a ritual, a repetitive behavior in response to the trigger, that are intended to prevent danger of which the obsession has created awareness and to diminish the responsibility for its possible occurrence, or to undo or neutralize things which may have already happened, that generates a sense of relief at that moment, these are called compulsions [26]. Also, if in observing the patient, there is no clear relationship between the obsession and the compulsion, another diagnosis should be considered [29]. Treating OCD entails seeking to break these rituals, and then exchanging the reward system for the discomfort.
Obsessive-Compulsive Disorder is biologically assumed as result from abnormalities in the serotonin pathway and dysfunctional circuits in the orbitostriatal area and the dorsolateral prefrontal cortex, while in the cognitive-behavioral aspect of the obsessive-compulsive disorder, emphasizes the importance of dysfunctional beliefs in affected individuals [30].
The World Health Organization, once ranked OCD in the top 10 of the most disabling illnesses by lost income and decreased quality of life, and also states the disorder as the sixth largest contributor to non-fatal health loss globally [31]. People with OCD are less likely to be married, are more likely to be unemployed, to subsist on very low incomes, and to have low occupational status [26]. When the prevalence and the functional impairment acting together with the anxiety and distress individuals with this condition experience are considered, one recognizes that OCD represents a significant public health concern [25].
OCD is often regarded as a very heterogeneous disorder, and is usually classified by grouping patients according to similarities in their symptoms [32, 33]. According to Bream [26], patients with OCD can be classified into four broad categories or subtypes of symptoms that may have different implications for causation and treatment: contamination fears, checking and other forms of verification, rumination, and also ordering and symmetry. Until recently considered as a part of OCD, the process of hoarding has been observed in a different number of phenomenological and outcomes variables, leading to its new status as a stand-alone disorder in DSM-V [28].
Two common pathways in the treatment of OCD are medications or Cognitive-Behavioral Therapy (CBT), particularly ‘Exposure with Response Prevention’ (ERP), and/or cognitive interventions aimed at specific obsession beliefs structures, or serotonin reuptake inhibitor (SRI) medications [25]. Currently, it is common practice and not very controversial to opt for psychotropic medication concomitantly with psychoanalysis. Studies have shown the combination of CBT with drugs such as clomipramine since the early 1980s, and fluvoxamine and imipramine since the 1990s [34].
Treatment employing CBT is presently associated with large effect sizes for both ERP and CBT tailored to the condition. Relative to psychotherapeutic interventions, SRI medications have somewhat lower effect sizes for symptom relief [25]. A significant minority fails to respond to the available treatments with estimates of non response as high as 30% [25].
Sufferers of OCD often have other psychopathologies, and tend to have a high level of comorbidity during their lifetime: anxiety disorders (76%), depressive or bipolar disorder (63%), major depressive disorder (41%), obsessive-compulsive personality disorder (23%–32%), tic disorder (30%) [28]. Other disorders that occur more frequently in individuals with OCD than those without the disorder, include several obsessive-compulsive and related disorders such as body dysmorphic disorder, trichotillomania (hair pulling disorder), and excoriation (skin-picking disorder) [28].
3 Cognitive-Behavioral Therapy - CBT
Cognitive-Behavioral Therapy (CBT) is a practice that has been developed and used since the 1970s [35], it is a rich, complex, and evolving model of treatment that has been developed for and applied to a wide range of mental health and physical problems and disorders [35], it is an active and directive approach used in the treatment of disorders such as depression, anxiety, phobias, among others [36].
According to Hofmann and Asmundson [37], it is not a single treatment protocol, instead, it refers to a family of interventions, as well as a scientific approach towards understanding and treating psychiatric disorders and human suffering [37]. CBT is among the most studied forms of psychotherapy [37, 38]. A description of the various CBT protocols easy fills a 3-volume textbook series [39] and it has demonstrated efficacy in the treatment of OCD [35].
The term CBT refers specifically to treatments that change cognitions (such as thoughts and beliefs) that are influencing psychological problems [40]. Beck [41] and Ellis [42] were the early theorists in what would become the field of CBT [35], they both developed models during the 1970s in which cognitive assessment and cognitive change became the pivotal point for later behavioral adaptation and emotional success [35].
Nowadays, there is a range of terms that can encompass the CBT practice. For example, ‘Behavior Therapy’ is also called as ‘Behavior Modification’ or ‘Cognitive-Behavioral Therapy’ [40]; ‘Cognitive Therapy’ - which has been developed by Beck [41] - can be called ‘Beckian CBT’, or ‘Formulation-Driven CBT’ [37]; and anything that falls under the rubric of CBT can be regarded as (general) ‘Rational Emotive Behavior Therapy - REBT’ [43] - which has been developed by Ellis [41]. Researchers also refer to the ‘Generic Cognitive Model of CBT’ as the ‘Case Formulation-Driven’ or ‘Case Conceptualization-Driven’ approach to CBT [44].
There are records of effective treatments for OCD both through an isolated cognitive or behavioral approach alone [45]. Some researchers may argue about the merits of using a strictly cognitive or strictly behavioral approach, however, more pragmatic therapists view cognitive and behavioral methods as effective partners in both theory and practice [46].
Economic data consistently show that the provision of CBT for common mental disorders is more cost-efficient than pharmacotherapy or other interventions such as psychodynamic therapies [37]. The Britain National Institute for Clinical Excellence (NICE) recommends CBT more often than other therapeutic approaches in the treatment of a variety of psychological disorders [43]. Also, the results of many outcome trials and academic researches demonstrate the efficacy of CBT psychological treatments [47], and specifically in the treatment of OCD [48], likewise CBT approaches are the most commonly cited among evidence-based psychological treatments [43].
CBT is also indicated to treat individuals with comorbidity, who are those patients diagnosed with more psychological diseases than OCD. They may benefit from receiving one course of a ‘Case Conceptualization-Driven’ approach to CBT as opposed to receiving several courses of treatment from different treatments protocols [49], furthermore, CBT appear to have roughly equivalent results across several therapies for common problems such as Major Depression Disorder (MDD) and addictions [47]. It is also recommended for the treatment of problems such as sleep disorders and many of the anxiety disorders - including panic, OCD, social anxiety, and posttraumatic stress disorder (PTSD) - as well as specific phobias [47]. Also, it is prudent to train clinicians working within a managed care setting to use this efficient approach to therapy across the comorbidity [37].
4 Games for Health - GfH
Games are artifacts deeply rooted in human social development and it is possible to draw a comparison between them and current rites and ceremonies [50]. Although many news media and scientific groups tend to focus just on the worst aspects of games, like apology of violence [51] and gaming vice [52], games can be used in several positive ways for the good of the individual and/or society. As examples of this positive outcome are Zelda [53], World of Warcraft [54] and Eve Online [55]. The first one can be used to teach children and teenagers basic concepts of scientific process through the game cycle - find a problem, observe, search the environment, formulate a solution (hypothesis) and test it [56]. The second one, contributed to the research of epidemiology, especially about simulating human reactions in high epidemic disease cases, when an in-game disease spread in the game in a non-intentional event called ‘Corrupted blood incident’ [57].
Using a slightly different approach, Eve Online developers partnered with Human Protein Atlas Project, Massively Multiplayer Online Science, and Reykjavik University, forming the project Discovery [58]. Developers created a mini-game within the game where the players could observe molecules from a microscope, and with little training, classify the molecule shown in the microscopic image. There was no obligation to any player to do it, it didn’t affect the gameplay, but those who actually did it were rewarded in in-game currency that could be used to buy spaceships and other in-game stuff.
Besides that, since the end of the 1970s and beginning of 1980s, many researchers and companies started to notice that the engaging power of games could be used to teach and/or train people [59]. This began what is today called ‘Serious Games’, but it didn’t stop just in the educational and training areas, spreading to several other areas like health systems, military, etc. In the words of Wattanasoontorn [60], there’s no common definition of Serious Games but, most researchers and developers agree that they are ‘games used for purposes other than mere entertainment’ [60].
When a serious game is used for health purposes, it can be called ‘Game for Health’ (GfH). The proper definition of this type of game crashes with multiple definitions of health concept [60]. Since health has several definitions, games for health have several applications and forms. However, looking at Sawyer and Smith [61]’s proposed game taxonomy; it is possible to verify the areas that games for health can encompass (as shown in Table 1).
The table columns divide the games by reasons to use and/or to make a GfH, while the rows divide the games by objectives within the health area. This bidimensional nature of the table allows an organic and flexible classification and, at the same time, shows how GfH’s can be different depending on how they are used. Nevertheless, it is important to point out that, because games are a complex media, the divisions proposed by this taxonomy are not mutually exclusive. As an example, an allergy disease management game also brings elements from self-ranking and first aid [62].
Another point of Sawyer and Smith’s taxonomy [61] is that it does not divide games by regular more usual game taxonomy, like platform type, or genre. That means it makes no difference if the game is digital or analogical, and, at the same time, it makes no difference if the game is an FPS (First Person Shooter), a board game, or a puzzle. Another very subtle or dubious type of game is the exergaming (and rehabilitation as consequence). Exergames are a type of game in which the player physically exercises while playing. To achieve that, a special device captures the player’s movements and transforms them into game input (commands). The term Exergames comes from the words ‘exercise and game’, but several publications make use of the term in a broader way, simply meaning, games where the player make commands using special devices. This way, from the point of view of this paper’s authors, it makes more sense to simply use ‘exercise’ instead of the term ‘exergaming’.
Wattanasoontorn [60] also developed taxonomy of games after surveying several publications in the area (as shown in Fig. 1).

Classification model proposed by Wattanasoontorn [60].
Wattanasoontorn’s [60] classification is more complex than the one developed by Sawyer and Smith [61]. The starting point is based on three points of views to classify the game - ‘Health’, ‘Player’, and ‘Serious Game/application’ (the game per se). Each of these points of view has their own subdivisions, grouping the classifications in clusters. Although more complex and more complete, this classification mode lacks some classifications like ‘research/academia’ and ‘public health’, that were found in Sawyer and Smith’s [61] model. This shows an interesting opportunity for further research and development but, for a while, this subject will be postponed since it is not entailed in the original scope of this research.
5 Literature Review
The purpose of this review of the literature is to summarize the previous published works and gather theoretical background material about using games as part of OCD treatment. Thus, the presentation is divided in two subsections: (i) Methodology, how the data was collected, selected, and analyzed; and (ii) Synthesis of the Literature Review, where the results were shown.
5.1 Methodology
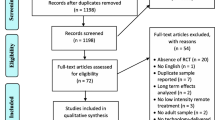
The methodology used in this review happened in two steps: the first one was to find papers about the use of games on OCD treatment; the second, to refine the search, analyzing and sorting the results. The online bibliographic research (desk research) had the following parameters: only papers written in English available in the search engine Google Scholar [63]. The search terms used were “OCD treatment” and “game”; all the searches occurred during the period between December 2018 and January 2019.
Using these parameters, we found 335 results in Google Scholar. However, due to the criteria of relevance and repetition in more than one source, the sampling for this work was110 sources collected for analysis. After an initial analysis, only papers of academic research were considered for having more updated information. Thus, 45 papers were selected for the literature review, as presented in the Appendix. The other sources, distributed in 30 books, 28 internet pages, 1 as citation, 2 as a result not found and 4 repeated in more than one source, can be used in the next works related to the subject of this review.
The second part of the analysis of the selected academic papers was also divided into two steps: the first one consisted in the selection of the papers that met the criteria required to compose the sample intended by this review, i.e., fulfill the cross-field between OCD and the use of games on its treatment, preferably by CBT. The second step was a thorough analysis of the articles selected to compose the sample.
On step 1, the selection of sources occurred according to the following criteria: (i) if the source dealt with OCD; (ii) if the therapy used was CBT; (iii) if the use of games during the process, whether digital or analog, was identified; (iv) if sources did not meet the previous criteria, identify the relationship of the content with the search keywords;
Step 2 comprised of the analysis of articles that somehow used games and dealt with the treatment of OCD by CBT by reading all the papers and identifying the following aspects: (i) basic characteristics of the patients, that is, and if the treatment consisted only of therapy, medications, or both; and whether patients were adults, children or adolescents; (ii) Identifying how the digital artifact was included in the treatment and if it was applied for diagnosis, treatment, prevention or metrics, and evaluations; (iii) in case of use of games, identifying whether they were analog or digital; if the paper dealt with an educational artifact, whether it was an active part in treatment or a motivational complement; whether developed for the work in analysis or an existing commercial game.
The collection and analysis of these data are intended to provide a glimpse of the actual development and use of games as a treatment for OCD.
5.2 Synthesis of the Literature Review
For a better understanding, the data analysis will be presented following the same pattern used in the methodology.
Step 1
When analyzing the 45 articles selected, 9 articles were extracted for a more in-depth analysis, since they met the criteria used in this review: games applied to the treatment of OCD, preferably by CBT. From the 9 (nine) articles [64,65,66,67,68,69,70,71,72], 8 (eight) met the criteria showed, and 1 (one) used ERP (exposure and response prevention), a therapy before CBT and that can be configured as one of its stages [73]. This ERP-based work was considered by similarity, but not selected for the sample later, because it did not contain use of game related to OCD.
Although there were 36 articles that did not meet the criteria for this research, they all went through a brief analysis to better understand the use of the term “game”, aiming at a macro view of this research. Besides these, 4 results appeared duplicated in the search engine and 2 were not found for analysis. 3 papers did not deal with OCD, CBT and, therefore, not related games, and in these cases, it was the word ‘game’ used in another context.
Out of the 36 papers that did not enter the sample, 32 dealt with OCD, 21 of them using CBT, 1 using ERP and 11 did not use either. For purposes of understanding these results, the following terms were established, and the number of articles using each one is indicated in parentheses: playful digital artifact or application to aid treatment (2); video game and/or internet Addiction (6); ‘game’ used in another context (14); gamification (3); games universe used in the construction of metaphors for the therapy (5); game as a recreational activity at some point in the session, after its completion or as homework (5); defended the possibility of games in VRET - Virtual Reality Exposure Therapy [74] and reasons for not having many cases (1);
When observing only the results of papers treating OCD by CBT (or ERP), there is a recurrence of terms only in the use of the game universe in the construction of metaphors for the therapy (4) [75,76,77,78]; gamification (3) [79,80,81]; playful digital artifact or application to aid treatment (2) [82, 83]; game as a recreational activity at some point in the session, after its completion or as homework (4) [84,85,86].
Step 2
The final sample, composed of the results that meet the research objectives of this review, has 9 results, 6 of which were applied in the treatment of children and/or adolescents, while 3 of adults. Only 2 used CBT and medications concomitantly for all patients, while 4 did not present a standard, having some medicated and others not, and one of the results did not show this information. The following items provide a preview of the 9 papers that make up the sample resulting from this review:
Brezinka, 2013 [64]
Development and evaluation of a therapeutic digital game to support OCD treatment. The game mentioned in the article was applied specifically for treatment of OCD. There is no information about the type of OCD treated. The game covered psycho-education, the cognitive model of obsessive compulsive disorder, creating a symptom hierarchy, the use of externalizing techniques to cope with anxiety and unpleasant feelings, and exposure-response prevention exercises. 18 children, 6–12 years, some patients received medication (16) and others did not (2). As results, Therapists perceived the game as helpful for education and enhance motivation. 93.75% of the patients evaluated presented remarkably less severe OCD, but there was no control group to validate the role of the game on therapy. In order to achieve success on game tasks, sometimes the Therapist’s or the parent’s motivation was needed. The game did not covered parents and siblings’ relation with the patient’s rituals, but the author explained the importance of Therapist help to reduce adaptation and even participation (from family) in the child’s rituals.
Comer, Furr, Cooper-Vince, Kerns, Chan, Edson, Khanna, Franklin, Garcia, and Freeman, 2014 [65]
Development of an Internet-based format for the delivery of family-based home-treatment for early-onset OCD. Real-time cognitive-behavioral therapy centering on exposure and response prevention to affected families through Video Conferencing and digital games. There is no information about the type of OCD treated. The game was played in session with parents and therapist to enhance the child understanding of treatment concepts. Games were both adaptations of previous works and new product created specifically for this experiment. 5 children, 4–8 years, none of the patients received medication. As results, all of the patients completed treatment and showed OCD symptom improvements and global severity improvements from pre- to post treatment, all showed at least partial diagnostic response, and 60% no longer met diagnostic criteria for OCD at post treatment. No participants got worse, the quality of services was perceived as ‘‘excellent.’’ by all parents involved. The games used for teaching core treatment content and for alliance building, highly engaged and motivate the children while working with the therapist.
Freeman, Garcia, Benito, Conelea, Khanna, March, and Franklin, 2012 [66]
Randomized trial to compare efficacy CBT and sertraline and their combination to a placebo control condition of the pediatric OCD treatment. Family-based CBT. Family-based relaxation therapy. There is no information about the type of OCD treated. At relaxation therapy the game was part of engagement strategies such as drawing and variants of preexisting the card games; at CBT, therapists made exposure into a game where possible (having fun, playing games, doing silly things in the presence of a feared stimulus). 127 children, of 7–17 years old, some patients received medication and others did not. As results, games were not mentioned, but as a result, this trial could contribute with information about the comparability of this treatment program with CBT, but given a time.
Haring and Warmelink, 2016 [67]
Case study of five psychotherapeutic games using metacognition (“third wave” of CBT). OCD was treated by one of the five games, named Ricky and the Spider [87], previously mentioned and already described at these results. The paper offers design recommendations for future (metacognitive) psychotherapeutic games in general.
Hong, Kim, Aboujaoude and Han, 2018 [68]
A serious game to support OCD treatment based on ERP approach, aiming at validating if the symptom improvement would be associated with altered Functional Connectivity within Cortico-striato-thalamo-cortical. 15 adults, none of the patients received medication. There is no information about the type of OCD treated. The game was meant to ask subjects to perform behaviors. Subjects played the game for at least 30 min per day, 5 days per week, for 3 weeks. The game was created and pre-tested specifically for this experiment. As results, the game was shown to improve OCD symptoms and alter brain connectivity from the dACC to the DLPFC and to basal ganglia. The author suggests serious games as a less expensive alternative than ERP and self-administrated.
Leib, 2001 [69]
Presents a multimodal method of treating OCD integrating psychoanalysis, psychopharmacology, and behavior modification. 1 adult received medication and CBT. The type of OCD was contamination fears. The game was mentioned at the sessions as of throwing things at each other to catch, a kind of exposure task through playing. There was neither digital nor board game. As results, the combined treatment was successful, but there is no mention about the use of game on it.
March, Mulle and Herbel, 1994 [70]
Development and evaluation of a treatment Manual designed to facilitate patient and parental compliance, exportability, and empirical evaluation. There is no information about the type of OCD treated. The game was used only to engage the child’s attention at the first session of therapy. 15 children and adolescents, all patients received medication. Because of its small contribution to treatment, the conclusions of the article did not mention the game, therefore, there are no relevant results about game on CBT.
Miller, 2008 [71]
FRIENDS is a developmental, linear, classroom-formatted group activity curriculum based on CBT principles, that includes lessons (10 sessions) on identification of feelings, relaxation, problem solving, challenging negative or unhelpful thoughts, and exposure activities. There is no information about the type of OCD treated and, although the article mentioned OCD, the project aimed at treating anxiety disorders in general. The game was a quiz only for the last session to review the content and have fun on the last day. 373 Children from one school and 6 children (symptomatic), grades 4 through 6, with no age description, during 10 week and no medication informed. Although FRIENDS is called a prevention program, the game used at lesson 10 was a review quiz among CBT steps. As results, the author presents society needs about anxiety prevention, school environment as convenient do deliver treatment, the need for more validation, but there is no mention about the use of the game.
Rocha, Alvarenga, Malloy-Diniz, and Corrêa, 2011 [72]
To evaluate the process of decision-making in patients with obsessive-compulsive disorder (OCD) using the Iowa Gambling Task (IGT), which is a card game. 214 adults (107 diagnosed with OCD and 107 healthy controls), some patients received medication (79) and others did not (22). There is inconsistent information about this sum, but it is registered here as it was in the original article. There is no information about the type of OCD treated. As results, the experiment found that OCD patients have significant deficits in their decision-making on the IGT, but also found that they performed equally well on several other tests that evaluate attention, different executive functions, memory and intelligence.
All outcomes that used game for educational purposes were intended for children and/or adolescents. And, of all results using games for educational purposes, only one was not developed for children and/or adolescents.
Concerning the use of digital artifact in relation to the treatment of OCD, 4 used it during the therapy sessions; 1 only at the end of the session; and 2 as homework; 2 did not use a digital artifact, but entered for analysis by using analog gaming. None of the 7 results using digital games was directed at prevention or diagnosis of OCD; however, 6 of them were used during the treatment and only 1 result recorded some type of metric.
About the use of games in relation to the sample, 8 of the 9 results, fulfilled the parameters aimed by this review, used game in the treatment of OCD by CBT. Among them, 5 applied a game developed specifically for this purpose and 4 applied commercial games, existing prior to the project. 1 result used game in the treatment of OCD by ERP.
Regarding the nature of the game and its positioning in the therapy, 4 of them were used for educational purposes; 6 as an active part in the treatment and one as a motivational complement, remembering that it is part of the beginning of the CBT, learning about OCD and its symptoms.
6 Final Conclusions
Veale and Roberts [24] say OCD is the fourth most common mental disorder. Its global prevalence is estimated between 1.2 to 3% of the general population [25]. Since worldwide population is around 7.5 billion [88], this prevalence corresponds to 90.6 to 226.5 millions of individuals suffering from OCD. This is roughly the population of countries like Germany (82.1 m), Mexico (129.1 m) and Pakistan (197 m) [88].
Since the fail rate of actual treatments is estimated as high as 30% [25], it means the window of improvement or search of alternative tools could improve the life of several million people around the globe. As games become more and more embedded in people’s daily lives, they become increasingly attractive for the development of Games for Health in general. Given the large number of people affected with OCD and who do not respond to current treatments, the games appear as a promising idea to be studied.
Some authors agree with the role of Game as a facilitator in OCD-directed Cognitive-Behavioral Therapy [80, 89]. From this literature review, starting from 110 results analyzed, only 9 results met the predefined parameters in the methodology. This review shows data that is contrary to the theoretical indications regarding the use of games in the CBT for treating OCD due to the small number of cases: 4 cases of games in general, 4 digital games and one did not mention whether it was digital or not. This is a small number considering the initial sample of 110 analyzed results. There is, therefore, potential for research in the area involving Games related to OCD.
Among the results analyzed, even the articles that did not come to compose the sample brought information to this research, such as the interest of professionals in the universe of games, appropriating metaphors for their therapy [75,76,77,78], or using Gamification in the CBT [79,80,81].
Regarding the use of games in the treatment of OCD by CBT, the concern of professionals in choosing this alternative when the therapy was aimed at children and adolescents was evident. This shows an open possibility for designers to reach these professionals evidencing relations of consumption of games by adults, aiming to expand the use for all the ages.
Concerning the possibility of choosing between using a commercial game [66, 69, 70, 72] or developing one specifically for the purpose [64, 65, 67, 68], although the results point to close numbers, it is important to draw attention here to the fact that the development of a game meant a considerable high cost for research until the beginning of the years 2000. The ease and lower costs can influence adherence to this type of solution in the coming years.
References
Kalapanidas, E., et al.: PlayMancer: games for health with accessibility in mind. Commun. Strat. 73, 105–120 (2009)
Ozcan, A.: Educational games for malaria diagnosis (2014)
Small, P., Pai, M.: Tuberculosis diagnosis - time for a game change (2010)
Freitas, D.Q., et al.: Development and evaluation of a kinect based motor rehabilitation game. In: Simpósio Brasileiro de Jogos e Entretenimento Digital. SBC, Brasil (2012)
Baranowski, T., Buday, R., Thompson, D.I., Baranowski, J.: Playing for real: video games and stories for health-related behavior change. Am. J. Prev. Med. 34(1), 74–82 (2008). https://doi.org/10.1016/j.amepre.2007.09.027
Bartolome, N.A., Zorrilla, A.M., Zapirain, B.G.: Can game-based therapies be trusted? Is game-based education effective? A systematic review of the Serious Games for health and education. In: IEEE Intelligent Systems, pp. 275–282. IEEE, New Jersey (2011)
Kharrazi, H., Lu, A.S., Ghargabi, F., Coleman, W.: A scoping review of health game research: Past, present, and future. Games Health Res. Dev. Clin. Appl. 1(2), 153–164 (2012). https://doi.org/10.1089/g4h.2012.0011
Mann, B.D., Eidelson, B.M., Fukuchi, S.G., Nissman, S.A., Robertson, S., Jardines, L.: The development of an interactive game-based tool for learning surgical management algorithms via computer. Am. J. Surg. 183(3), 305–308 (2002)
Sodre, C., Costa, A., Apolinário, J., Barros, F., Santos, A.: The metabolic race: an educational game. Revista de Ensino de Bioquímica 16(7) (2018)
Sietsema, J.M., Nelson, D.L., Mulder, R.M., Mervau-Scheidel, D., White, B.E.: The use of a game to promote arm reach in persons with traumatic brain injury. Am. J. Occup. Ther. 47(1), 19–24 (1993)
Vedamurthy, I., et al.: A dichoptic custom-made action video game as a treatment for adult amblyopia. Vis. Res. 114, 173–187 (2015)
Brown, S.J., Lieberman, D.A., Gemeny, B.A., Fan, Y.C., Wilson, D.M., Pasta, D.J.: Educational video game for juvenile diabetes: results of a controlled trial. Med. Inform. 22(1), 77–89 (1997). https://doi.org/10.3109/14639239709089835
Lieberman, D.A.: Management of chronic pediatric diseases with interactive health games: theory and research findings. J. Ambul. Care Manage. 24(1), 26–38 (2001)
Kapp, K.M.: The Gamification of Learning and Instruction: Game-based Methods and Strategies for Training and Education. Wiley, Hoboken (2012)
Prins, P.J.M., Dovis, S., Ponsioen, A., Ten Brink, E., Van der Oord, S.: Does computerized working memory training with game elements enhance motivation and training efficacy in children with ADHD? Cyberpsychol. Behav. Soc. Networking 14(3), 115–122 (2011)
Gardner, J.E.: Can the Mario Bros. help? Nintendo games as an adjunct in psychotherapy with children. Psychother. Theor. Res. Pract. Train. 28(4), 667 (1991)
Brezinka, V.: Treasure Hunt-a serious game to support psychotherapeutic treatment of children. Stud. Health Technol. Inform. 136, 71 (2008)
Coyle, D., Matthews, M.: Personal investigator: a therapeutic 3D game for adolescent psychotherapy. Interact. Technol. Smart Educ. 2(2), 73–88 (2005). https://doi.org/10.1108/1741565058000034
Brown, S.J.: Method for treating medical conditions using a microprocessor-based video game. U.S. Patent No 5,918,603 (1999)
Wilkinson, N., Ang, R.P., Goh, D.H.: Online video game therapy for mental health concerns: a review. Int. J. Soc. Psychiatry 54(4), 370–382 (2008)
Gamberini, L., Barresi, G., Majer, A., Scarpetta, F.: A game a day keeps the doctor away: a short review of computer games in mental healthcare. J. CyberTher. Rehabil. 1(2), 127–146 (2008)
Luxton, D.D., McCann, R.A., Bush, N.E., Mishkind, M.C., Reger, G.M.: mHealth for mental health: Integrating smartphone technology in behavioral healthcare. Prof. Psychol. Res. Pract. 42(6), 505 (2011)
Ayuso-Mateos, J.L.: Global burden of obsessive-compulsive disorder in the year 2000. World Health Organization. Global Burden Disease 2000, Draft 21-08-06 (2000)
Veale, D., Roberts, A.: Obsessive-compulsive disorder. BMJ 348, g2183 (2014)
Abramowitz, J.S., McKay, D., Storch, E.A.: The Wiley Book of Obsessive-Compulsive Disorder, vol. 1. Wiley, Hoboken (2017)
Bream, V., Challacombe, F., Palmer, A., Salkovskis, P.: Cognitive Behaviour Therapy for Obsessive-Compulsive Disorder. Oxford University Press, Oxford (2017)
Sasson, Y., Zohar, J., Chopra, M., Lustig, M., Iancu, I., Hendler, T.: Epidemiology of obsessive-compulsive disorder: a world view. J. Clin. Psychiatry 58(12), 7–10 (1997)
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edn. American Psychiatric Association, Arlington (2013)
Franklin, M.E., Harrison, J., Benavides, K.: Treatment of childhood tic disorders with comorbid OCD. In: Storch, E., McKay, D. (eds.) Handbook of Treating Variants and Complications in Anxiety Disorders, pp. 135–148. Springer, New York (2013). https://doi.org/10.1007/978-1-4614-6458-7_9
Abramowitz, J.S., Taylor, S., Mckay, D.: Obsessive-compulsive disorder. Lancet 374(9688), 491–499 (2009)
OCD—UK. https://www.ocduk.org/ocd/world-health-organisation/. Accessed 11 Dec 2018
Baer, L.: Standardized assessment of personality disorders in obsessive-compulsive disorder. Arch. Gen. Psychiatry 47(9), 826–830 (1990)
Leckman, J.F., et al.: Symptoms of obsessive-compulsive disorder. Am. J. Psychiatry 154(7), 911–917 (1997). https://doi.org/10.1176/ajp.154.7.911
Van Balkom, A.J.L.M., Van Oppen, P., Vermeulen, A.W.A., Van Dyck, R., Nauta, M.C.E., Vorst, H.C.M.: A meta-analysis on the treatment of obsessive compulsive disorder: A comparison of antidepressants, behavior, and cognitive therapy. Clin. Psychol. Rev. 14(5), 359–381 (1994). https://doi.org/10.1016/0272-7358(94)90033-7
Wenzel, A., Dobson, K.S., Hays, P.A.: Cognitive Behavioral Therapy Techniques and Strategies. American Psychological Association, Washington, DC (2016)
Beck, A.T.: Cognitive Therapy of Depression. Guilford press, New York (1979)
Hofmann, S.G., Asmundson, G.J.G.: The Science of Cognitive Behavioral Therapy. Academic Press, Elsevier, Cambridge (2017). http://dx.doi.org/10.1016/B978-0-12-803457-6.00001-5
Butler, A.C., Chapman, J.E., Forman, E.M., Beck, A.T.: The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin. Psychol. Rev. 26(1), 17–31 (2006). https://doi.org/10.1016/j.cpr.2005.07.003
Hofmann, S.G.: The Wiley Handbook of Cognitive Behavioral Therapy, 1st edn. Wiley, New Jersey (2014). https://doi.org/10.1002/9781118528563.wbcbt01
Spiegler, M.D., Guevremont, D.C.: Contemporary Behavior Therapy, 5th edn. Wadsworth, Cengage Learning, Belmont (2010)
Beck, A.T.: Cognitive therapy: nature and relation to behavior therapy. Behav. Ther. 1, 184–200 (1970). https://doi.org/10.1016/S0005-7894(70)80030-2
Ellis, A., Whiteley, M.M.: Theoretical and Empirical Foundations of Rational-emotive Therapy. Brooks/Cole, Monterey (1979)
Dryden, W.: Rational Emotive Behavior Therapy, 1st edn. Routhledge, East Sussex (2009)
Persons, J.B.: The Case Formulation Approach to Cognitive-behavor Theraphy. Guilford Press, New York (2008)
Chosak, A., Marques, L., Fama, J., Renaud, S., Willhelm, S.: Cognitive therapy for obsessive-compulsive disorder: A case example. Cogn. Behav. Pract. 16(1), 7–17 (2009). https://doi.org/10.1016/j.cbpra.2008.01.005
Wright, J.H., Basco, M.R., Thase, M.E.: Aprendendo a Terapia Cognitivo-comportamental. Artmed Editora, Porto Alegre (2009)
Dobson, D., Dobson, K.S.: Evidence-Based Practive of Cognitive-Behavioral Therapy, 2nd edn. Guilford Press, New York (2017)
Storch, E.A., et al.: Does cognitive-behavioral therapy response among adults with obsessive–compulsive disorder differ as a function of certain comorbidities? J. Anxiety Disord. 24(6), 547–552 (2010)
Persons, J.B.: Case formulation-driven psychotherapy. Clin. Psychol. Sci. Pract. 13(2), 167–170 (2006)
Huizinga, J.: Homo Ludens: O Jogo Como Elemento da Cultura. Editora Perspectiva, São Paulo (2001)
Goldbeck, L., Pew, A.: Violent video games and aggression. http://www.center4research.org/violent-video-games-can-increase-aggression/. Accessed 17 Dec 2018
Ng, B.D., Wierner-Hastings, P.: Addiction to the internet and online gaming. CyberPsychol. Behav. 8(2), 110–113 (2005). https://doi.org/10.1089/cpb.2005.8.110
Zelda. https://www.zelda.com/. Accessed 16 Nov 2018
Wow. https://worldofwarcraft.com/pt-br/. Accessed 16 Nov 2018
Eve. https://www.eveonline.com/. Accessed 16 Nov 2018
Johnson, S.: Tudo o que é ruim é bom para você. Zahar, Rio de Janeiro (2012)
Orland, K.: GfH: the real life lessons of wow’s corrupted blood, 20 May 2018. https://www.gamasutra.com/php-bin/news_index.php?story=18571. Accessed 18 Feb 2018
Kelly, A.: How Eve Online players are helping medical science, 26 Apr 2016. https://www.pcgamer.com/how-internet-spaceships-are-helping-medical-science/. Accessed 22 Dec 2018
Prensky, M.: Aprendizagem Baseada em Jogos Digitais. Editora Senac, São Paulo (2012)
Wattanasoontorn, V., Boada, I., García, R., Sbert, M.: Serious Games for Health. Entertainment Comput. 4, 231–247 (2013)
Sawyer, B., Smith, P.: Serious games taxonomy. https://thedigitalentertainmentalliance.files.wordpress.com/2011/08/serious-games-taxonomy.pdf. Accessed 22 Dec 2018
de Vasconcellos, M.S., de Carvalho, F.G., Capella, M.A.M., Dias, C.M., de Araujo, I.S.: A Saúde na Literatura Acadêmica sobre Jogos: uma análise das publicações do SBGames. In: SBC – Proceedings of XV SBGames, SBC, Brasil, São Paulo (2016)
Google Scholar. https://scholar.google.com. Accessed 27 Jan 2019
Brezinka, V.: Ricky and the spider: a video game to support cognitive behavioral treatment of children with obsessive-compulsive disorder. Clin. Neuropsychiat. 10(3) (2013)
Comer, J.S., et al.: Internet-delivered, family-based treatment for early-onset ocd: a preliminary case series. J. Clin. Child Adolesc. Psychol. 43(1), 74–87 (2014)
Freeman, J., et al.: The pediatric obsessive compulsive disorder treatment study for young children (pots jr): developmental considerations in the rationale, design, and methods. J. Obsessive-compulsive Relat. Disord. 1(4), 294–300 (2012)
Haring, Priscilla, Warmelink, Harald: Looking for Metacognition. In: Bottino, Rosa, Jeuring, Johan, Veltkamp, Remco C. (eds.) GALA 2016. LNCS, vol. 10056, pp. 95–106. Springer, Cham (2016). https://doi.org/10.1007/978-3-319-50182-6_9
Hong, J.S., Kim, S.M., Aboujaoude, E., Han, D.H.: Investigation of a mobile “serious game” in the treatment of obsessive–compulsive disorder: a pilot study. Games Health J. 7(5), 317–326 (2018). https://doi.org/10.1089/g4h.2017.0158
Leib, P.T.: Integrating behavior modification and pharmacotherapy with the psychoanalytic treatment of obsessive-compulsive disorder: a case study. Psychoanal. Inquiry 21(2), 222–241 (2001)
March, J.S., Mulle, K., Herbel, B.: Behavioral psychotherapy for children and adolescents with obsessive-compulsive disorder: an open trial of a new protocol-driven treatment package. J. Am. Acad. Child Adolesc. Psychiatry 33(3), 333–341 (1994)
Miller, L.D.: Facing fears: The feasibility of anxiety universal prevention efforts with children and adolescents. Cogn. Behav. Pract. 15(1), 28–35 (2008)
da Rocha, F.F., Alvarenga, N.B., Malloy-Diniz, L., Corrêa, H.: Decision-making impairment in obsessive-compulsive disorder as measured by the iowa gambling task. Arqu. Neuropsiquiatr. 69(4), 642–647 (2011)
Havnen, A., Hansen, B., Haug, E.T., Prescott, P., Kvale, G.: Intensive group treatment of obsessive-compulsive disorder: a pilot study. Clin. Neuropsychiatry 10(3) (2013)
Aboujaoude, E., Salame, W., Naim, L.: Telemental health: a status update. World Psychiatry 14(2), 223–230 (2015)
Cassano, M.C., Nangle, D.W., O’Grady, A.C.: Exposure-based treatment for a child with stabbing obsessions. Clin. Case Stud. 8(2), 139–157 (2009)
Wu, M.S., Storch, E.A.: Personalizing cognitive-behavioral treatment for pediatric obsessive-compulsive disorder. Expert Rev. Precis. Med. Drug Dev. 1(4), 397–405 (2016)
Abramowitz, J.S., Blakey, S.M., Reuman, L., Buchholz, J.L.: New directions in the cognitive-behavioral treatment of ocd: theory, research, and practice. Behav. Ther. 49(3), 311–322 (2018). https://doi.org/10.1016/j.beth.2017.09.002
Herren, J., Brannan, E.: Clinical considerations for implementing exposure and response prevention for pediatric ocd. Univ. Child Adolesc. Behav. Lett. 34(6), 1–7 (2018)
Sloman, G.M., Gallant, J., Storch, E.A.: A school-based treatment model for pediatric obsessive-compulsive disorder. Child Psychiatry Human Dev. 38(4), 303–319 (2007)
Peterman, J.S., Read, K.L., Wei, C., Kendall, P.C.: The art of exposure: putting science into practice. Cogn. Behav. Pract. 22(3), 379–392 (2015). https://doi.org/10.1016/j.cbpra.2014.02.003
Wilson, R., Neziroglu, F., Feinstein, B.A., Ginsberg, R.: A new model for the initiation of treatment for obsessive–compulsive disorder: an exploratory study. J. Obsessive-compulsive Relat. Disord. 3(4), 322–337 (2014). https://doi.org/10.1016/j.jocrd.2014.08.003
Whiteside, S.P.H., Ale, C., Vickers, K.S., Tiede, M.S., Dammann, J.E.: Case examples of enhancing pediatric OCD treatment with a smartphone application. Clin. Case Stud. 13(1), 80–94 (2014)
Matthews, A.J., Maunder, R., Scanlan, J.D., Kirkby, K.C.: Online computer-aided vicarious exposure for OCD symptoms: A pilot study. J. Behav. Ther. Exp. Psychiatry 54, 25–34 (2017). https://doi.org/10.1016/j.jbtep.2016.06.002
Foa, E.B., McLean, C.P.: The efficacy of exposure therapy for anxiety-related disorders and its underlying mechanisms: the case of ocd and ptsd. Annu. Rev. Clin. Psychol. 12, 1–28 (2016)
Neziroglu, F., Fruchter, Y.: Manifestation and treatment of ocd and spectrum disorders within a pediatric population. Anxiety Disorders-From Childhood to Adulthood (2018)
Bouchard, S., Mendlowitz, S.L., Coles, M.E., Franklin, M.: Considerations in the use of exposure with children. Cogn. Behav. Pract. 11(1), 56–65 (2004). https://doi.org/10.1016/S1077-7229(04)80007-5
Rick and the Spider. https://rickandthespider.uzh.ch. Accessed 15 Jan 2019
UN: World Population Prospects 2017. Data Booklet (2017)
Brezinka, V.: Computer games supporting cognitive behaviour therapy in children. Clin. Child Psychol. Psychiatry 19(1), 100–110 (2014)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Appendix
Appendix
-
1.
Aboujaoude, E., Salame, W., Naim, L.: Telemental health: a status update. World psychiatry 14(2), 223–230 (2015).
-
2.
Abramowitz, J. S., Blakey, S. M., Reuman, L., Buchholz, J.L.: New directions in the cognitive-behavioral treatment of ocd: theory, research, and practice. Behavior therapy 49(3), 311–322 (2018). https://doi.org/10.1016/j.beth.2017.09.002
-
3.
An, S. K., Mataix-Cols, D., Lawrence, N. S., Giampietro, V., Speckens, A., Brammer, M. J., Phillips, M. L.: To discard or not to discard: the neural basis of hoarding symptoms in obsessive-compulsive disorder. Molecular psychiatry 14(3), 318 (2009). https://doi.org/10.1038/sj.mp.4002129
-
4.
Bipeta, R., Yerramilli, S. S. R. R., Karredia, A. R., Gopinath, S.: Diagnostic stability of Internet addiction in obsessive-compulsive disorder: Data from a naturalistic one-year treatment study. Innovations in clinical neuroscience 12(3–4), 14–23 (2015).
-
5.
Boger, K., Sperling, J., Potter, M., Gallo, K. P.: Treatment overview of an intensive group outpatient cognitive-behavioral therapy for youth anxiety disorders and obsessive-compulsive disorder. Evidence-Based Practice in Child and Adolescent Mental Health 1.2(3), 116–125 (2016). https://doi.org/10.1080/23794925.2016.1227947
-
6.
Bouchard, S., Mendlowitz, S. L., Coles, M. E., Franklin, M.: Considerations in the use of exposure with children. Cognitive and behavioral practice 11(1), 56–65 (2004). https://doi.org/10.1016/s1077-7229(04)80007-5
-
7.
Brezinka, V.: Ricky and the spider: a video game to support cognitive behavioral treatment of children with obsessive-compulsive disorder. Clinical Neuropsychiatry 10(3) (2013).
-
8.
Cassano, M. C., Nangle, D. W., O’Grady, A. C.: Exposure-based treatment for a child with stabbing obsessions. Clinical Case Studies 8(2), 139–157 (2009).
-
9.
Comer, J. S., Furr, J. M., Cooper-Vince, C. E., Kerns, C. E., Chan, P. T., Edson, A. L., Khanna, M., Franklin, M. E., Garcia, A. M., Freeman, J. B.: Internet-delivered, family-based treatment for early-onset ocd: a preliminary case series. Journal of Clinical Child & Adolescent Psychology 43(1), 74–87 (2014).
-
10.
Cusimano, A.: Emdr in the treatment of adolescent obsessive-compulsive disorder: a case study. Journal of EMDR Practice and Research 12(4), 242–254 (2018).
-
11.
Drake, K. L., Ginsburg, G. S.: Family-based cognitive-behavioral treatment of chronic pediatric headache and anxiety disorders: a case study. Child & Youth Care Forum. 579–598 (2012).
-
12.
Falkenstein, M. J., Mouton-Odum, S., Mansueto, C. S., Goldfinger, G., Haaga, D. A. F.: Comprehensive behavioral treatment of trichotillomania: a treatment development study. Behavior modification 40(3), 414–438 (2016). https://doi.org/10.1177/0145445515616369
-
13.
Foa, E. B., McLean, C. P.: The efficacy of exposure therapy for anxiety-related disorders and its underlying mechanisms: the case of ocd and ptsd. Annual review of clinical psychology 12, 1–28 (2016).
-
14.
Freeman, J., Garcia, A., Benito, K., Conelea, C., Sapyta, J., Khanna, M., March, J., Franklin, M.: The pediatric obsessive compulsive disorder treatment study for young children (pots jr): developmental considerations in the rationale, design, and methods. Journal of obsessive-compulsive and related disorders 1(4), 294–300 (2012).
-
15.
Hammond, D. C.: Neurofeedback with anxiety and affective disorders. Child and Adolescent Psychiatric Clinics 14(1), 105–123 (2005).
-
16.
Haring, P., Warmelink, H.: Looking for metacognition. International Conference on Games and Learning Alliance. 95–106 (2016).
-
17.
Havnen, A., Hansen, B., Haug, E. T., Prescott, P., Kvale, G.: Intensive group treatment of obsessive-compulsive disorder: a pilot study. Clinical Neuropsychiatry 10(3), (2013).
-
18.
Herren, J., Brannan, E.: Clinical considerations for implementing exposure and response prevention for pediatric ocd. The Brown University Child and Adolescent Behavior Letter 34(6), 1–7 (2018).
-
19.
Hong, J. S., Kim, S. M., Aboujaoude, E., Han, D. H.: Investigation of a mobile “serious game” in the treatment of obsessive–compulsive disorder: a pilot study. Games for health journal 7(5), 317–326 (2018). https://doi.org/10.1089/g4h.2017.0158
-
20.
Kalra, S. K., Swedo, S. E.: Children with obsessive-compulsive disorder: are they just “little adults”?. The Journal of clinical investigation 119(4), 737–746 (2009).
-
21.
Kendall, P. C., Beidas, R. S.: Smoothing the trail for dissemination of evidence-based practices for youth: flexibility within fidelity. Professional Psychology: Research and Practice 38(1), (2007).
-
22.
Leib, P. T.: Integrating behavior modification and pharmacotherapy with the psychoanalytic treatment of obsessive-compulsive disorder: a case study. Psychoanalytic Inquiry 21(2), 222–241 (2001).
-
23.
Lovato, L., Ferrão, Y. A., Stein, D. J., Shavitt, R. G., Fontenelle, L. F. Vivan, A., Miguel, E. C., Cordioli, A. V.: Skin picking and trichotillomania in adults with obsessive-compulsive disorder. Comprehensive psychiatry 53(5), 562–568 (2012).
-
24.
Majchrzak, J. D.: Creative therapy in treating adolescent obsessive-compulsive disorder: a proposed therapeutic treatment. Meeting of Minds XVI Journal of Undergraduate Research 10, 107 (2003).
-
25.
March, J. S., Mulle, K., Herbel, B.: Behavioral psychotherapy for children and adolescents with obsessive-compulsive disorder: an open trial of a new protocol-driven treatment package. Journal of the American Academy of Child & Adolescent Psychiatry 33(3), 333–341 (1994).
-
26.
Matthews, A. J., Maunder, R., Scanlan, J. D., Kirkby, K. C.: Online computer-aided vicarious exposure for OCD symptoms: A pilot study. Journal of behavior therapy and experimental psychiatry 54, 25–34 (2017). https://doi.org/10.1016/j.jbtep.2016.06.002
-
27.
Miller, L. D.: Facing fears: The feasibility of anxiety universal prevention efforts with children and adolescents. Cognitive and Behavioral Practice 15(1), 28–35 (2008).
-
28.
Neziroglu, F., Fruchter, Y.: Manifestation and treatment of ocd and spectrum disorders within a pediatric population. Anxiety Disorders-From Childhood to Adulthood. (2018).
-
29.
O’Neill, J., Schwartz, J.: The role of volition in ocd therapy: neurocognitive, neuroimaging, and neuroplastic aspects. Clinical Neuropsychiatry 1(1), 13–31 (2004).
-
30.
Osgood-Hynes, D., Belmont, M. A.: Thinking bad thoughts. MGH/McLean OCD Institute.
-
31.
Peterman, J. S., Read, K. L., Wei, C., Kendall, P. C.: The art of exposure: putting science into practice. Cognitive and behavioral practice 22(3), 379–392 (2015). https://doi.org/10.1016/j.cbpra.2014.02.003
-
32.
Rocha, F. F. da, Alvarenga, N. B., Malloy-Diniz, L., Corrêa, H.: Decision-making impairment in obsessive-compulsive disorder as measured by the iowa gambling task. Arquivos de Neuro-psiquiatria 69(4), 642–647 (2011).
-
33.
Rosa, A. C., Diniz, J. B., Fossaluza, V., Torres, A. R., Fontenelle, L. F., de Matthis, A. S., Rosário, M. da C., Miguel, E. C., Shavitt, R. G.: Clinical correlates of social adjustment in patients with obsessive-compulsive disorder. Journal of psychiatric research 46(10), 1286–1292 (2012). https://doi.org/10.1016/j.jpsychires.2012.05.019
-
34.
Rowicka, M. Internet addiction treatment. Gambling and Internet Addictions: Epidemiology and Treatment. 55–64, (2016).
-
35.
Sloman, G. M., Gallant, J., Storch, E. A.: A school-based treatment model for pediatric obsessive-compulsive disorder. Child psychiatry and human development 38(4), 303–319 (2007).
-
36.
Tavares, H., Gentil, V.: Pathological gambling and obsessive-compulsive disorder: towards a spectrum of disorders of volition. Revista Brasileira de Psiquiatria 29(2), 107–117 (2007).
-
37.
Thomsen, P. H.: Obsessive-compulsive disorder in children and adolescents. Clinical guidelines. European child & adolescent psychiatry 7(1), 1–11 (1998).
-
38.
Tolin, D. F.: Alphabet soup: erp, ct, and act for ocd. Cognitive and Behavioral Practice 16(1), 40–48 (2009).
-
39.
Valerio, C., Diniz, J. B., Fossaluza, V., de Mathis, M. A., Belotto-Silva, C., Joaquim, M. A., Miguel Filho, E. C., Shavitt, R. G.: Does anti-obsessional pharmacotherapy treat so-called comorbid depressive and anxiety states?. Journal of affective disorders 139(2), 187–192 (2012). https://doi.org/10.1016/j.jad.2012.02.002
-
40.
Weidle, B., Skarphedinsson, G.: Treatment of a child with obsessive compulsive disorder with limited motivation: course and outcome of cognitive behavior therapy. Journal of clinical psychology 72(11), 1139–1151 (2016).
-
41.
Wetherell, J. L.: Treatment of anxiety in older adults. Psychotherapy: Theory, Research, Practice, Training 35(4), 444 (1998).
-
42.
Whiteside, S. P. H., Ale, C., Vickers, K. S., Tiede, M. S., Dammann, J. E.: Case examples of enhancing pediatric OCD treatment with a smartphone application. Clinical Case Studies 13(1), 80–94 (2014).
-
43.
Wilson, R., Neziroglu, F., Feinstein, B. A., Ginsberg, R.: A new model for the initiation of treatment for obsessive–compulsive disorder: an exploratory study. Journal of Obsessive-Compulsive and Related Disorders 3(4), 322–337 (2014). https://doi.org/10.1016/j.jocrd.2014.08.003
-
44.
Wilson, R. R.: The anxiety disorder game. Psychotherapy in Australia 12(2), 36–45 (2006).
-
45.
Wu, M. S., Storch, E. A.: Personalizing cognitive-behavioral treatment for pediatric obsessive-compulsive disorder. Expert Review of Precision Medicine and Drug Development 1(4), 397–405 (2016).
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this paper

Cite this paper
Miranda, J., Teofilo, V., Lins, A., Oliveira, B.S., Campos, F., Nesteriuk, S. (2019). Literature Review: The Use of Games as a Treatment for Obsessive Compulsive Disorder. In: Duffy, V. (eds) Digital Human Modeling and Applications in Health, Safety, Ergonomics and Risk Management. Healthcare Applications. HCII 2019. Lecture Notes in Computer Science(), vol 11582. Springer, Cham. https://doi.org/10.1007/978-3-030-22219-2_38
Download citation
DOI: https://doi.org/10.1007/978-3-030-22219-2_38
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-22218-5
Online ISBN: 978-3-030-22219-2
eBook Packages: Computer ScienceComputer Science (R0)