
Abstract
Dental anxiety has become one of the most important problems affecting patients’ timely consultation and visiting experience. The purpose of this study is to help patients who have the emotion of dental anxiety to relieve anxiety by a virtual reality product based on computerized cognitive behavioral therapy. The study collected MDAS, GSR, and HRV data of 24 adults with dental anxiety through experiments to evaluate the degree of dental anxiety, and evaluated the user experience by user experience questionnaire. According to the data analysis, MDAS, GSR, and HRV has been decreased after the intervention, which confirmed the effectiveness of the virtual reality dental anxiety mitigation tool based on computerized cognitive behavioral therapy. At the same time, direct exposure to the virtual dental environment also has certain utility, but the effect is not equal to the former.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Dental anxiety is one of the most important factors influencing the patient’s dental experience. Because of the phobia of pain and dental treatment equipment such as dental drills, fear of unknown things, or terrible dental treatment experience in childhood, some people are caught in a negative emotion of dental anxiety. Dental anxiety makes patients unable to cooperate with dentists. Delay treatment or even refuse to see a doctor. Statistically, dental anxiety afflicts a significant proportion as high as 50%, with 6%–20% of patients who have severe dental anxiety [1]. Therefore, reliable and timely management of the negative emotions is necessary to improve oral health and life quality for the people who are experiencing dental anxiety.
2 Literature Review
2.1 Dental Anxiety
A growing number of scholars and dentists are aware of the adverse effects of dental anxiety on oral health, and have carried out a series of researches on dental anxiety. They explore the means of assessing dental anxiety and the factors affecting dental anxiety, with the intention of finding ways to relieve dental anxiety. Those effective ways can be applied in clinical practice. Psychological intervention and drug treatment have proven to be effective in alleviating dental anxiety at present. Psychological intervention such as cognitive behavioral therapy, exposure therapy, music therapy, aromatherapy, relaxation and distraction have been increasingly used in the practice of oral treatment with the advantage of no side effect.
Here comes the overview of some psychological intervention methods and their advantages and disadvantages (Table 1).
2.2 Cognitive Behavioral Therapy
Cognitive behavioral therapy (CBT) is widely used in the practice of dental anxiety through cognitive reorganization, knowledge education, Psychological counseling and relaxation. Mihaela (2014) examined the effectiveness of cognitive behavioral therapy in reducing dental anxiety. Four sessions of cognitive restructuring technique were used in order to reduce the dental anxiety level. Compared with the control group without any intervention, substantial reductions of dental trait anxiety could be obtained through sessions of cognitive restructuring [2]. Tellez (2015) developed a cognitive-behavioral protocol based on psychoeducation, exposure to feared dental procedures, and cognitive restructuring. This computer based tool was confirmed to be efficacious in reducing dental anxiety [5].
However, as a psychological intervention, limitations of cognitive behavioral therapy are also significant. This method requires full follow-up by researchers, dentists or professional psychologists. Moreover, CBT personnel need to undergo rigorous training, which requires a lot of human resources and needs a fixed training location.
Therefore, more auxiliary therapies such as reading therapy and computerized cognitive behavior therapy are developed based on modern technology and resources.
Computerized cognitive behavior therapy can effectively reduce the occupation of professional resources and suggest to be efficacious in alleviating dental anxiety. In recent years, scholars combine cognitive behavior theory with design science furtherly. The interdisciplinary research bridges the deficiencies of traditional cognitive behavior therapy.
2.3 Virtual Reality
With the real-time performance feedback, self-guided exploration and independent practice, low-cost environment that can be duplicated and distributed, virtual reality enables patients to achieve remote self-training in the field of medical, which greatly saves resources. In the field of medical treatment, virtual reality has been widely used in psychotherapy, cognitive rehabilitation, mental disorders and auxiliary training [14,15,16,17]. It also has a good effect on relieving anxiety caused by fear. For example, combining exposure therapy and virtual reality can effectively relieve acrophobia, social phobia and preoperative anxiety [18, 19]. On the other hand, it is also an effective way to provide a relaxing environment in virtual reality to help patients escape from the horrible reality [11].
To this end, this study firstly summarized the existing literature, analyzed the characteristics of the people who are experiencing dental anxiety. Then the whole study developed a relief tool for dental anxiety in virtual reality environment based on serious game and cognitive behavioral therapy, and explored a new type of computerized cognitive behavior therapy framework based on virtual reality. The purpose is to help patients with evasion and fear of oral treatment to relieve their negative emotions and improve their treatment experience (Table 2).
3 Materials and Methods
3.1 System Design
Before completing the specific design, the research investigated the reasons of dental anxiety, and determined the horror gradient of the dental clinic scene. It is found that negative associations with dental treatment, insufficient awareness of dental diseases, fear of unknown treatments and barriers to communicate with dentists become the main causes of anxiety. The result will guide subsequent designs.
Four virtual dental treatment scenarios with increasing horror levels are developed according to the research:
-
1)
A dental environment with dental instruments and a virtual dentist surrounding the participant.
-
2)
The virtual dentist with a dental mirror in his hand moves towards to the participant, just like doing an oral examination.
-
3)
The virtual dentist with a dental syringe in his hand moves towards to the participant, just like doing an oral therapy.
-
4)
The virtual dentist with a dental drill in his hand moves towards to the participant, just like doing an oral therapy.
The experiment was performed in a quiet room of 5 m * 3 m. The seat simulates the height and angle of a dental seat. The VR helmet uses HTC VIVE, including a helmet, two handles and two lighthouses. The program is developed by Unity 2018.3.10 and runs in SteamVR.
Experimental Group (VR-CBT).
The VR-CBT group will present a narrative and easy-to-understand interpretation of the dentist’s upcoming treatment before each scene. Participants can autonomously control the course of treatment according to their own adaptation.
Control Group (VR).
The VR group will only be presented in the same 4 virtual scenes as the VR-CBT group (Figs. 1 and 2).

The virtual reality dental anxiety mitigation product design. (Left: the scene design; Right: the scene from the patient’s perspective.)

The introduction to the upcoming virtual treatment in the form of a pop-up window in the experimental group.
3.2 Participants
24 participants who were about to visit a dentist were recruited in order to verify the effectiveness of computerized cognitive-behavioral therapy in virtual reality. All participants were asked to sign a consent and fill out a subjective basic information questionnaire before the experiment. The inclusion criteria are as follow: 1) Participants with a MDAS score ≥15; 2) Participants who don’t have hearing or visual impairments, known balance disorders, post-traumatic stress disorder, developmental or intellectual disability. 3) Participants have never received any cognitive behavioral therapy treatment for their dental anxiety in the past.
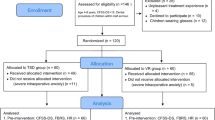
3.3 Procedure
A total of 24 samples were tested in the single-blind experiment, with 12 participants in the experimental group and 12 participants in the control group. First of all, participants should filling the modified dental anxiety scale. Then they were asked to wear the physiological testing equipment in order to get their galvanic skin response and heart rate. After that, a video about tooth extraction was provided to determine their baseline of dental anxiety. Participants both in the experimental group and control group then wore the VR helmet for the text. At the same time, quantitative intervention results were obtained during the text.
After the experiment, participants could remove the physiological testing equipment and the VR helmet, then filled out the modified dental anxiety scale again and filled out the user experience questionnaire.
3.4 Measurements
Modified Dental Anxiety Scale (MDAS).
The modified dental anxiety scale is a common measure of dental anxiety which is effective in assessing dental anxiety in an internationally diverse sample. The scale consists of five indicators: 1) If you went to your Dentist for treatment tomorrow, how would you feel? 2) If you were sitting in the waiting room (waiting for treatment), how would you feel? 3) If you were about to have a tooth drilled, how would you feel? 4) If you were about to have your teeth scaled and polished, how would you feel? 5) If you were about to have a local anaesthetic injection in your gum, above an upper back tooth, how would you feel?
Each indicator is divided into five levels with a score from 1 to 5: 1) Not Anxious 2) Slightly Anxious 3) Fairly Anxious 4) Very Anxious 5) Extremely Anxious. The total score ranges from 5 to 25 points, and usually 15 points is the threshold for mid-to-high dental anxiety [20].
Galvanic Skin Response (GSR).
GSR measurements work by detecting the changes in electrical ionic activity resulting from changes in sweat gland activity. It is found that galvanic skin response can respond to anxiety. A statistically significant correlation was found between galvanic skin conductance and dental anxiety. Advantageously, combining with GSR measurements during the experiment can quantify patients’ anxiety. Caprara measured patients’ dental fear scale, GSC and polygraph response to key verbal questions, finally verified that dental anxiety can be measured objectively by skin conductance [21].
Heart Rate (HR).
Heart rate can reflect the patient’s anxiety during oral treatment. When people feel stress or anxiety, a series of responses come out, such as increased heart rate, blood pressure, blood sugar, and dilated pupils. Heart rate is usually included in the evaluation index when measuring the degree of dental anxiety.
In the study, Brand Psytech were used to collect galvanic skin response and heart rate data.
User Experience Questionnaire (UEQ).
User experience questionnaire was used to evaluate a preferably comprehensive impression of the product user experience from the six aspects of attractiveness, perspicuity, efficiency, dependability, stimulation, and novelty.
4 Result
4.1 MDAS
After the F-test, this study used an independent sample T-test to verify whether the baseline levels of dental anxiety in the experimental group and the control group were consistent. The result shows that there is no significant difference in the degree of dental anxiety between the experimental group and the control group (p = 0.792 > 0.05). The samples are statistically significant (Fig. 3).

Independent samples text of MDAS (group 1: experimental group; group 2: control group).
Moreover, the study used paired-samples T-test to compare the self-reported differences in dental anxiety between the experimental and control groups. There are four sets of MDAS data: the experimental group’s pre-text (Mean = 17.75) and post-text (Mean = 14.33), the control group’s pre-text (Mean = 17.42) and post-text (Mean = 15.83). The data shows that the degree of self-reported dental anxiety decreased in both groups after the experiment. there is a significant difference between the pre-test and post-test in the experimental group (p = 0.002 < 0.01), and there has a difference between the pre-test and post-test in the control group, but the difference was not significant. (P = 0.027 < 0.05) The data above proves the effectiveness of the virtual reality dental anxiety mitigation tool based on computerized cognitive behavioral therapy. At the same time, direct exposure to the virtual dental environment also has certain utility (Fig. 4).

Paired samples text of MDAS.
4.2 SC/GSR
Figure 5 shows one typical participant’s GSR, BVP and HR trend which are measured with biosignal recorder during the experiment. It is found that as the experiment progresses, the participant’s GSR decreasing gradually.

One typical participant’s GSR, BVP and HR trend during the experiment.
Furtherly, the study used paired-samples T-text to analyze the changes between the pre-text and post-text of the experimental group and control group after confirming that there is no significant difference in the degree of the galvanic skin response between the experimental group and the control group before the experiment. The first 30 s of the experiment was selected as the pre-test data, and the last 30 s of the experiment was used as the post-test data. The data shows that both experimental group and control group have a significant difference (experimental group: p = 0.003 < 0.05, control group: p = 0.004 < 0.05) (Fig. 6).

Paired samples text of GSR (group 1: experimental group’s pre-text; group 2: experimental group’s post-text; group 3: control group’s pre-text; group 4: control group’s post-text).
The research furtherly used a scatter plot to analyze whether the difference is reflected in relieving or increasing anxiety. In the scatter plot, the pre-text is used as the independent variable, and the post-test is used as the dependent variable. According to the chart, most of the scattered points are below the line y = x. The significant difference is reflected in relieving the dental anxiety. Scilicet, the participants in the two groups’ dental anxiety level decreased after using the product (Fig. 7).

The scatter plot of the experimental group (left) and control group (right).
Moreover, an independent sample T-test was used to compare the difference of GSR between the experimental group and the control group (p = 0.138 > 0.05). It can be seen that the design of the two groups can alleviate the level of anxiety, but the difference between the two groups is not significant.
4.3 HRV
The study used paired-samples T-test to analyze the differences between the time-domain index RMSD and SDNN of the heart rate variability between the experimental group and the control group (Fig. 8).

Paired samples text of HRV
In terms of RMSSD, there is a significant difference between the experimental group’s pre-text and post-test (p = 0.019 < 0.05) while there is no significant difference between the control group’s pre-text and post-test (p = 0.098 > 0.05). And in terms of SDNN, there is a significant difference between the experimental group’s pre-text and post-test (p = 0.002 < 0.05) while there is no significant difference between the control group’s pre-text and post-test (p = 0.119 > 0.05).
4.4 UEQ
The study combines the user experience questionnaire to evaluate the user experience of product design from the six aspects of attractiveness, perspicuity, efficiency, dependability, stimulation, and novelty. In general, the user experience of the experimental group is better than that of the control group. And the product design of the experimental group is more prominent in three aspects of attractiveness, novelty and perspicuity. These three aspects have a significant difference between the two groups (Figs. 9 and 10).

Independent samples text of UEQ (group 1: experimental group; group 2: control group).

The mean value and standard deviation of the UEQ’s six aspect (experimental group: figure left; control group: figure right).
5 Discussion
It is found that participants had higher levels of dental anxiety before intervention. The anxiety level of experimental group and control group are both decreased after intervention. And the anxiety level of VR-CBT group was significantly lower than that of the control group. This demonstrates the effectiveness of cognitive behavioral therapy combined with virtual reality, while also finding that exposing patients to virtual reality environments directly also plays a role. Compared with exposure therapy under virtual reality, cognitive behavioral therapy in virtual reality environment is obviously more effective, and the result shows that the user experience of the VR-CBT group is better than the control group especially in terms of attractiveness, novelty and perspicuity. In addition, combined with the MDAS and GSR index before and after the experiment, the correlation between the GSR and dental anxiety emotions can be verified.
This study is an interdisciplinary research in the field of health care and industrial design. It provides a virtual reality product design to release dental anxiety that can be used at home. The first advantage of the design lies in the vivid dentistry environment that virtual reality simulated. It can let patients who tend to delay or refuse to see a doctor adjust their mood remotely and seek medical advice timely, and the treatment experience becomes better accordingly. Secondly, computerized cognitive behavioral therapy based on virtual reality can replace oral imparting experience. By the time, it allows patients to control the treatment process autonomously and professional therapists will be no longer needed. This is a new practice of virtual reality in the field of medical, which has certain practical significance and clinical value. The study shows that computerized cognitive behavioral therapy combined with virtual reality is an effective method to alleviate the emotion of anxiety in dental treatment. However, there are still some limitations. The experiment belongs to a short-term experiment, which can only test state anxiety but do not reflect the effects of long-term trait anxiety. In the future, the sample size will be expanded and long-term intervention will be included.
References
Kleinknecht, R.A., Klepac, R.K., Alexander, L.D.: Origins and characteristics of fear of dentistry. J. Am. Dent. Assoc. 86(4), 842–848 (1973)
Dumitrache, M.A., Neacsu, V., Sfeatcu, I.R.: Efficiency of cognitive technique in reducing dental anxiety. Procedia Soc. Behav. Sci. 149, 302–306 (2014). https://doi.org/10.1016/j.sbspro.2014.08.246
Haukebø, K., et al.: One- vs. five-session treatment of dental phobia: a randomized controlled study. J. Behav. Ther. Exp. Psychiatry 39(3), 381–390 (2008). https://doi.org/10.1016/j.jbtep.2007.09.006
Matsuoka, H., Chiba, I., Sakano, Y., Toyofuku, A., Abiko, Y.: Cognitive behavioral therapy for psychosomatic problems in dental settings. BioPsychoSocial Med. 11(1) (2017). Article number: 18. https://doi.org/10.1186/s13030-017-0102-z
Tellez, M., et al.: Computerized tool to manage dental anxiety. J. Dent. Res. 94(9_suppl), 174S–180S (2015). https://doi.org/10.1177/0022034515598134
Lehrner, J., Marwinski, G., Lehr, S., Johren, P., Deecke, L.: Ambient odors of orange and lavender reduce anxiety and improve mood in a dental office. Physiol. Behav. 86(1), 92–95 (2005). https://doi.org/10.1016/j.physbeh.2005.06.031
Venkataramana, M., Pratap, K., Padma, M., Kalyan, S., Reddy, A.A., Sandhya, P.: Effect of aromatherapy on dental patient anxiety: a randomized controlled trial. J. Indian Assoc. Public Health Dent. 14(2), 131 (2016)
Di Nasso, L., Nizzardo, A., Pace, R., Pierleoni, F., Pagavino, G., Giuliani, V.: Influences of 432 Hz music on the perception of anxiety during endodontic treatment: a randomized controlled clinical trial. J. Endod. 42(9), 1338–1343 (2016). https://doi.org/10.1016/j.joen.2016.05.015
Mejía-Rubalcava, C., Alanís-Tavira, J., Mendieta-Zerón, H., Sánchez-Pérez, L.: Changes induced by music therapy to physiologic parameters in patients with dental anxiety. Complement. Ther. Clin. Pract. 21(4), 282–286 (2015). https://doi.org/10.1016/j.ctcp.2015.10.005
Neacsu, V., Sfeatcu, I.R., Maru, N., Dumitrache, M.A.: Relaxation and systematic desensitization in reducing dental anxiety. Procedia Soc. Behav. Sci. 127, 474–478 (2014). https://doi.org/10.1016/j.sbspro.2014.03.293
Tanja-Dijkstra, K., et al.: Can virtual nature improve patient experiences and memories of dental treatment? A study protocol for a randomized controlled trial. Trials 15(1), 90 (2014). https://doi.org/10.1186/1745-6215-15-90
Gujjar, K.R., van Wijk, A., Kumar, R., de Jongh, A.: Efficacy of virtual reality exposure therapy for the treatment of dental phobia in adults: a randomized controlled trial. J. Anxiety Disord. 62, 100–108 (2019). https://doi.org/10.1016/j.janxdis.2018.12.001
Gujjar, K.R., van Wijk, A., Kumar, R., de Jongh, A.: Are technology-based interventions effective in reducing dental anxiety in children and adults? A systematic review. J. Evid. Based Dent. Pract. 19(2), 140–155 (2019). https://doi.org/10.1016/j.jebdp.2019.01.009
Pandrangi, V.C., Gaston, B., Appelbaum, N.P., Albuquerque, F.C., Levy, M.M., Larson, R.A.: The application of virtual reality in patient education. Ann. Vasc. Surg. 59, 184–189 (2019). https://doi.org/10.1016/j.avsg.2019.01.015
Scozzari, S., Gamberini, L.: Virtual reality as a tool for cognitive behavioral therapy: a review. In: Brahnam, S., Jain, L.C. (eds.) Advanced Computational Intelligence Paradigms in Healthcare 6. SCI, vol. 337, pp. 63–108. Springer, Heidelberg (2011). https://doi.org/10.1007/978-3-642-17824-5_5
Yang, Y.-C.: Role-play in virtual reality game for the senior. Association for Computing Machinery, Aizu-Wakamatsu (2019)
Yu, J., Jiang, R., Feng, Y., Yuan, M., Kang, Y.I., Gu, Z.: Mobile VR game design for stroke rehabilitation. In: Rau, P.-L.P. (ed.) CCD 2018. LNCS, vol. 10912, pp. 95–116. Springer, Cham (2018). https://doi.org/10.1007/978-3-319-92252-2_8
Sanchez, A.Y.R., Kunze, K.: Flair: towards a therapeutic serious game for social anxiety disorder. Paper Presented at the Proceedings of the 2018 ACM International Joint Conference and 2018 International Symposium on Pervasive and Ubiquitous Computing and Wearable Computers, Singapore (2018)
Thanh, V.D.H., Pui, O., Constable, M.: Room VR: a VR therapy game for children who fear the dark. Paper Presented at the SIGGRAPH Asia 2017 Posters, Bangkok, Thailand (2017)
Humphris, G.M., Morrison, T., Lindsay, S.: The modified dental anxiety scale: validation and United Kingdom norms. Community Dent. Health 12(3), 143–150 (1995)
Caprara, H.J., Eleazer, P.D., Barfield, R.D., Chavers, S.: Objective measurement of patient’s dental anxiety by galvanic skin reaction. J. Endod. 29(8), 493–496 (2003). https://doi.org/10.1097/00004770-200308000-00001
Acknowledgement
The research is supported by National Social Science Fund (Grant No. 18BRK009).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this paper

Cite this paper
Han, T., Xiao, H., Shen, T., Xie, Y., Zhu, Z. (2020). A Virtual Reality Dental Anxiety Mitigation Tool Based on Computerized Cognitive Behavioral Therapy. In: Chen, J.Y.C., Fragomeni, G. (eds) Virtual, Augmented and Mixed Reality. Industrial and Everyday Life Applications. HCII 2020. Lecture Notes in Computer Science(), vol 12191. Springer, Cham. https://doi.org/10.1007/978-3-030-49698-2_26
Download citation
DOI: https://doi.org/10.1007/978-3-030-49698-2_26
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-49697-5
Online ISBN: 978-3-030-49698-2
eBook Packages: Computer ScienceComputer Science (R0)