
Abstract
Playing is part of children’s daily life and it is an important aspect of their development because it promotes not only entertainment, but also influences the psychological, physiological and social development of children. The playful aspect of the toys awakens other interests in Children with Disabilities (CwD), encouraging them to set aside their limitations. However, they are often prevented from playing because the toys are not accessible. Studies also show that the adoption of accessible toys can be an effective resource in CwD rehabilitation treatment. Thus, this work presents the results of a Systematic Review that investigated methods, techniques and interaction strategies used for coeiving and/or adapting accessible toys for CwD. In the context of this research, accessible and interactive toys are named Inclusive Toys (IT). The results of this SR allowed researchers to formulate hypotheses from the interaction and automation resources identified, to specify a model for the conception and design of IT supported by PD techniques.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Playing is part of children’s daily life. It is an important role in their development, promoting entertainment, and also influencing the children’s psychological, physiological and social development. Furthermore, it favors learning in different aspects of daily life, including that of Children with Disabilities (CwD), since they can explore their body and the environment with the toy [11, 12, 16].
In addition, the playful aspect of the toys awakens other interests in CwD, encouraging them to set aside their limitations. However, they cannot often play because toys are not accessible. It is highlighted that an accessible toy allows CwD to play freely, as it provides them with the necessary independence to playing and also to interact with other children, improving social interaction.
Studies also show that the adoption of accessible toys can be an effective resource in the CwD rehabilitation treatment [12, 16]. Additionally, the literature presents the creation of intelligent toys, automated and adapted to various purposes [11], but they are still poor in relation to accessibility for CwD [16, 17].
Therefore, this work is part of a larger context, which aims to investigate accessibility aspects and interaction resources to design automated toys with an accessible interface for CwD in order to assist in the therapeutic treatment. It aims to present the results of a Systematic Review (SR), which investigated the interaction strategies and automation resources used in the design and/or adaptation of accessible toys for CwD. In the context of this research, accessible and interactive toys are named Inclusive Toys (IT), because include children in playful resources.
2 Methodology
The methodology of investigation applied in this study was the SR process from the literature, based on a searching strings combination, varying the database IEEE, ACM and Google Scholar, trying to answer the following research questions:
-
(1)
What methods and interaction and automation techniques have been studied and applied to development or adaptation of IT supporting the therapeutic treatment of rehabilitation of CwD?
-
(2)
What techniques and/or methods are used to develop and to design IT?
During the preliminary selection, the works included in and excluded from the SR were defined according to the inclusion and exclusion criteria established in the protocol of the Systematic Review.
Figure 1 presents a flowchart with the different phases arising from SR, based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [10]. This flowchart aims to quantitatively present the SR process, from the initial identification of studies, using searches in databases, to the final selection of articles included in the data analysis.

Distribution of studies included in and excluded from the Systematic Review.
As observed in Fig. 1, 139 studies were found by applying search strings. In the preliminary selection phase, 29 articles were selected, out of which only 16 articles were included in the final SR selection. These articles sought to answer the research questions posed in the SR protocol.
3 Results of Systematic Review
The following paragraphs present a summary of the 16 articles analyzed. Each of the articles was individually analyzed. These studies represent the first steps of the study, and also render a deeper understanding of the context of the investigation, since they present accessibility aspects and interaction resources to design automated accessible IT in order to assist CwD in therapeutic treatment.
Nine out of the 16 works selected presented IT researches for children with autism (Sect. 3.1) and the other works presented IT researches for CwD with different disabilities (Sect. 3.2).
A synthesis of the interaction strategies and of the automation resources identified in each study included in the SR is presented in Table 1. Sections 3.1 and 3.2 present a summary of each work so as to understand the contribution of each study.
3.1 IT for Children with Autism
In the field of autism, Andreae et al. [1] propose developing a social robot (Active Auti) equipped with sensors and built according to the Applied Behavior Analysis (ABA) principles, aiming to stimulate the social behavior of children with Autism Spectrum Disorder (ASD), encouraging them to behave positively and discouraging them from negative behavior. The robot acts as a social assistant and has pre-programmed actions that will be executed according to the physical and verbal behavior of children with ASD. Note that the authors emphasize the preference of children with autism for objects, which makes robots an optimal alternative for entertainment.
The work by Qidwai et al. [14] also aims to develop/adapt toys for autistic children. The authors propose an IT with a source of light or audio, since these resources attract the attention of children with autism. The toys are equipped with remote control and are initially controlled by the child’s caretaker since, according to the authors, a child with autism may resist using the remote control at the first contact. However, after an adaptation period, with the caretaker’s support, the control can be an acceptable device. In this study, the authors used a PS2 remote control (Playstation 2 with vibration), a notebook and a (robotic) toy.
Another study on IT for children with autism is presented by Mazzei et al. [9], who propose a humanoid robot named FACE, able to express different emotions and to promote empathy with the patient. The robot is applied to adaptive therapy sessions, and is assigned the role of a social assistant, in which the robot adapts to the needs and learning skills of each patient. The robot is equipped with cameras and the child that will have the movements imitated wears a microphone, a shirt, a cap and an eyepatch; the latter three items are equipped with sensors. The FACE robot is able to copy a limited number of facial expressions; those most accepted by children with autism are selected. The interaction of the robot with the patient is direct and spontaneous.
Ranatunga et al. [15] also present a robot called ZENO para children with autism following a social assistant approach, which seeks to gradually improve the imitation (in this case, the patient imitates the robot that reproduces the movements of the human therapist) and the social interaction of the patient by means of adaptive training. The authors proposed a framework that makes the logical communication of the therapist’s movements captured by Kinect (Xbox 360/ONE movement sensor) and sends them to the robot. The ZENO robot reproduces the movements made by the human therapist, because the speed of the human being movements may not be in agreement with the motor skills of the child with autism. Therefore, it is possible to control the speed of the robot’s articulations, allowing the movements to be performed slowly. According to the authors, abrupt movements tend not to be accepted by children with autism.
An architecture mediated by robots aiming to develop an individualized and adaptable robotic therapeutic platform, especially for children with autism is presented by Esubalew et al. [2]. This platform aims to manage joint attention (of all those involved) and to conduct a usability study investigating the potential of ASD intervention mediated by robots and, therefore, makes a social assistant approach. The system comprises two monitors hanging from specific places, able to provide visual and audio stimuli. These include images of interest to the children (children’s characters) and video or audio with similar contents. Initially, the robot waits for the child to interact; in case the interaction fails, the robot seeks to stimulate the child using videos and images.
Huijnen et al. [7] present a framework designed for the social interaction of children with autism, tested in the KASPAR robot, developed by the same research group [6]. The KASPAR robot may perform body movements or gestures using the hands, arms, torso, head, as well as facial expressions (demonstrate emotions). The robot, allied to the framework, seeks to stimulate the child as from movements, sounds, expressions and miming, and can also formulate words, both for answering and for talking, in case the child does not react.
Another study involving a robot, Soleiman et al. [18] provides a social interactive robot approach (called RoboParrot), designed to provide comfort and emotional interaction to autistic children. The robot has a controller connected to a camera and to an embedded system, comprising different parts, such as the body-engine, head-engine, an Infra-Red (IR) sensor, a touch sensor, a microphone and a speaker (from where the RoboParrot’s voice is emitted). The robot is controlled by a remote operator, who can be an autism expert. The control has a camera so that the operator can see/interact with the child. The robot has several articulations in the body parts, enabling it to perform a number of movements.
The robot also uses its microphone, IR sensor and its speaker for the operator to communicate with the child. The head/body sensors are used to determine which part of the Parrot’s body the child is interacting with. RoboParrot is based on the Hasbro Toy CompanyFootnote 1 toy, and an embedded system has been added, connected to the toy as from a USB and DATA BUS.
The Mobile Robot proposed by Goulart et al. [5], was implemented to stimulate the autist child’s attention and its ability to interact with the environment, aiding in the social evolution process. It uses another robot as a base, the Pioneer 3 DX, which has an autonomous mechanism, programmed to have safety rules and a control system for planning and locomotion interaction. Considering that the robot interacts according to its environment, the system was programmed so that interactions with the environment generate inputs in axes x and y (accounting for moving the Mobile Robot), which will consequently generate action controls. A video camera, touchscreen, multimedia system, laser (to detect the distance from the robot to objects/wall) and Pioneer (accounting for the movements) were employed.
Boccanfuso and O’Kane [3] highlight that interactive and imitation games have yielded positive results for autistic children when they have difficulties in communication or social skills. The authors present the development of a robot, the approach of which focuses on integrating games and robots. Charlie, an acronym for Child-Centered Adaptive Robot for Learning in an Interactive Environment, was developed to be used as an imitation game, by means of tracking the movements of the hands and head. The cameras and movement sensors are coupled to the robot, which was trained to detect human hands. Two types of games were developed: single-player (“Imitate Me, Imitate You”) and tow-player (“Pass the Pose”). Furthermore, a third way of playing was added to the robot, which is remotely controlled.
3.2 IT for Children with Different Disabilities
Hengeveld et al. [6] propose developing an educational system, with interactive and adaptive learning that stimulate the language skills of children with multiple disabilities aged 1 to 4 years (toddlers), presenting a methodology to develop and to adapt a toy, game and/or a system for CwD.
According to the authors, when designing an artifact for such young children and with multiple disabilities, we must first consider interfaces different from the traditional Graphical User Interface (GUI), seeing that children under normal development acquire language skills apparently effortlessly and mainly playing. Children are observed to usually explore their environment physically and, by interacting with more experienced colleagues or adults, they seek help. Hence, the authors suggest Tangible User Interfaces (TUIs) as a design platform, due to the benefits of the physical contact of TUIs [6].
Note that the physical objects require less interpretation; they reduce the speed of interaction, which benefits this interaction; it allows a more flexible style of interaction and provides opportunities for collaborative use; it promotes and stimulates the interaction among the parts interested (children). Thus, making the interaction tangible allows offering children with multiple disabilities a type of sensorial experience rarely found in a ludic physical environment [6].
The work by Ljunglöf et al. [8] presents the development of a toy robot (Lekbot) and of a communication board to be used by physical, cognitive or communication PwD, including children. The communication board acts as a fun alternative, allowing CwD to communicate. The interaction occurs by selecting figures, stimulating the communication between child and toy. Next, the word is reproduced by synthesized voice via communication board, as a response to the interaction between child and the “toy”. The robot is equipped with sensors and interacts with the child by using voice and movements in the articulations. It additionally counts on self-learning in the way of correctly pronouncing words. These two computational solutions (communication board and robot) aim to improve the CwD trust and to promote language development, focusing on interaction strategies (verbal communication, touchscreen and sensors). The study was applied to children presenting cerebral palsy and complex difficulty in communication.
Colombo et al. [4] developed a plush dolphin (Dolphin Sam) aiming to help children with Intellectual Disability (ID) to learn by playing and by digitally interacting with the physical toy. The toy is based on practices used in the Dolphin Therapy (DT) – an animal therapy technique. The toy was built with sensors, actuators and external components. The toy benefit is to increase basic cognitive, emotional and social skills not much developed in children with ID. The dolphin was designed to increment the following skills: reach a relaxed state of mind; exercise attention (audio and visual signs); understanding the cause-effect relationship; exercising control and making daily choices.
As regards adapting controls and toys, Thaller and Nussbaum [19] developed an alternative control interface, approaching a social therapy, so as to control toys making them accessible to children with motor disability, so that it can promote the development of the children’s motor and cognitive skills. The first prototype was based on Arduino, developed for a tetraplegic patient, restricted to head and forearm movements. Sensors were coupled to the patient’s shoulders for sending information to the 4D Joystick which was also developed. The prototype evolution process followed user-centered approach.
Murphy et al. [11] propose “playground” for socializing humans with robots to include a number of children with different disabilities, making playing more sociable, interactive and attractive. The framework incorporates low-cost robots and toys, which employ infrared sensors, thermometer and microphone for monitoring the child’s health, detecting, for example, allergic reactions or changes in body temperature.
A sensorial platform is proposed by Proença et al. [13], to control toys for children with multiple disabilities to use. The aim of this platform is to receive stimuli from the CwD to control toys easily and flexibly during the rehabilitation process. The control is a Personal Digital Assistant (PDA) which child interacts with as from physical contact, by touching buttons. The child receives the feedback by means of visual stimuli in the device/control.
Vega-Barbas et al. [20] present an intelligent toy totally built and equipped with sensors to assess the psychomotor development in children up to 6 years of age. The goal was to design, to develop and to assess the toy usability do to facilitate the children’s health monitoring process. The authors propose methods to develop a toy from the collection of requirements, stressing that, as there are currently different technologies to make a toy inclusive, the authors propose a general methodology to develop a toy adapted to CwD. The interaction methods applied are sounds, lights and vibrations. A smartphone or tablet is used to control the toy. The authors highlight that, for tests, the proposal should be applied to children up to six years of age.
4 Discussion
The SR first research question showed that 50% of the studies included used adapted robots or Personal Digital Assistant to support the CwD development related to communication and social interaction skills [1, 3, 4, 8, 11]. Other studies proposed that some toys, such as helicopter, dolls, were be adapted by using remote control to assist the CwD in their different needs [13, 14, 19, 20].
Most of these studies used shelf toys and common robots that were adapted, seeking to reduce customization costs. In these toys, some automation devices are assembled, such as motors, sensors and actuators. Also, cameras, tablets, mobile phones and network interfaces were connected to allow controlling the toy remotely, besides transmitting collected data for remote processing. The studies generally examined the use of adapted toys in therapeutic treatment for different kinds of disability (cognitive, physical, social) and highlighted the importance of creating interaction strategies to improve the accessibility of toys.
It should be highlighted that the recent advances of embedded computing and of the Internet of Things have helped people to create toys that interact with local networks and these advances provide easy ways for these people to control these adapted toys or a program new functionalities.
Regarding the second research question, we did not find methodologies or models to develop and to design IT. The studies were verified to include techniques of Participatory Design (PD) in the SR, which are not part of the adaptation process of toys. Note that PD as an active involvement methodology of users in the adaptation process is fundamental to customize toys, allowing the active participation of CwD as co-designers of their solution.
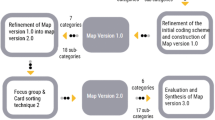
As a proposal of a PD methodology to treat this disability in the literature, we suggest that, in the process of creating a new inclusive toy or of adapting an existing toy, the model proposed and presented in Fig. 2 is adopted. It anticipates the participation of different actors in the IT creation/adaptation process, among which we detach health professionals (doctors, physiotherapists, therapists, nurses), the very child (patient), parents, caretakers, engineers, 3D device designers and programmers.

Model proposed for building IT with the participation of the different actors in the process
In Fig. 2, parents/caretakers and health professionals are observed to be able to define the way of stimulating the ludic side of CwD. Together with that, the participation of engineers and computer scientists help to model the technical aspects of the toy construction, especially combining the techniques used for developing objects related to the Internet of Things (IoT).
The refinement of the toy considering an interdisciplinary team including the different stakeholders of the process may help by delimiting the scope of the toy, as well as contributing to its evolution. This is because the technical team depends on the knowledge and on the experience of health professionals, caretakers and the very patient. All these actors may contribute to the PD, acting as co-designers for building the computational solution, providing the necessary know-how and learning with the other collaborators, so as to minimize failures and to favor improvement opportunities.
Hence, the goal of the model proposed (Fig. 2) is to contribute with an IT development process with the participation of the different actors in the process, to make it efficient regarding the therapeutic and ludic aspects. It has to manage to entertain the children and to make them feel immersed in the toy, but concurrently, as is deemed necessary, allows it to be intelligent and permits capturing data, including the children’s behavior when interacting with the toy.
The model proposed herein is supported on the strong points and limitations found in the different works identified in the SR. We observed that the interdisciplinary collaboration in the ITs design or adaptation process is essential to build computational solutions for including CwD in society. Aligned with the goal of this study, which seeks to include CwD to ludic resources, the model proposed aims to systemize the toy construction and the customization process, especially by bringing therapists, parents, caretakers and children to participate in the process.
The model thus highlights the importance of interdisciplinarity in the construction of an interactive and ludic computational solution for CwD, considering the view of the different areas involved in the process. Moreover, it contemplates a continuous improvement process in the IT construction/adaptation, considering the feedback of the potential users, as new data are collected and assessed.
5 Conclusion
As already mentioned, although accessible toys present the potential to be an effective resource in CwD rehabilitation treatment, they are still poor in relation to accessibility for CwD. This research reaches its goals by investigating this problem and recognizing the importance of contributing, cooperating to this focus by presenting the results of a SR that investigated methods, techniques and interaction strategies using the design/or adaptation of accessible toys for CwD.
Thus, the results of this SR allowed researchers to formulate hypotheses from the interaction and automation resources identified, to specify the interaction and accessibility requirements for toys adaptation and to specify a model for the conception and design of Inclusive Toys with the support of the PD techniques. The solutions proposed herein can contribute to the health area, extending the toy industry and related areas that make use of this feature.
We stress that, according to the results, one of the relevant future research points to case studies including CwD, therapists, caretakers, programmers and engineers, in rehabilitation institutions and hospitals. The aim is to conceive IT adapted to CwD in their rehabilitation treatment, following the approach of the model proposed herein.
Another future relevant work is evaluating the accessibility aspects and interaction resources identified in the RS, by means of practical cases and applying IT to potential users, in this case, Children with Disabilities, supported by their health professionals and caretakers.
We highlight that other possibilities arise to improve the inclusion of CwD in the social environment. Investigating more accessible interaction techniques so as to include CwD in society is therefore strongly recommended.
Notes
References
Andreae, H.E., Andreae, P.M., Low, J., Brown, D.A.: Study of auti: a socially assistive robotic toy. In: Proceedings of the 2014 Conference on Interaction Design and Children, pp. 245–248. ACM, New York (2014). http://doi.org/10.1145/2593968.2610463
Bekele, E.T., Lahiri, U., Swanson, A.R., Crittendon, J.A., Warren, Z.E., Sarkar, N.: A step towards developing adaptive robot-mediated intervention architecture (ARIA) for children with autism. IEEE Trans. Neural Syst. Rehabil. Eng. 21(2), 289–299 (2013). https://doi.org/10.1109/TNSRE.2012.2230188
Boccanfuso, L., O’Kane, J.M.: CHARLIE: an adaptive robot design with hand and face tracking for use in autism therapy. Int. J. Soc. Robot. 3(4), 337–347 (2011)
Colombo, S., Garzotto, F., Gelsomini, M., Melli, M., Clasadonte, F.: Dolphin Sam: a smart pet for children with intellectual disability. In: Proceedings of the International Working Conference on Advanced Visual Interfaces, pp. 352–353. ACM, New York (2016). http://doi.org/10.1145/2909132.2926090
Goulart, C.M., Castillo, J., Valadao, C.T., Caldeira, E., Bastos-Filho, T.F.: Mobile robotics: a tool for interaction with children with autism. In: IEEE International Symposium on Industrial Electronics, pp. 1555–1559 (2014). https://doi.org/10.1109/ISIE.2014.6864846
Hengeveld, B., Voort, R., Hummels, C., Overbeeke, K., Balkom, L., Moor, J.: LinguaBytes. In: Proceedings of the 7th International Conference on Interaction Design and Children, pp. 17–20 (2008). https://doi.org/10.1145/1463689.1463707
Huijnen, C.A.G.J., Lexis, M.A.S., de Witte, L.P.: Matching robot KASPAR to autism spectrum disorder (ASD) therapy and educational goals. Int. J. Soc. Robot. 8(4), 445–455 (2016)
Ljunglöf, P., Claesson, B., Müller, I. M., Ericsson, S., Ottesjö, C., Berman, A., Kronlid, F.: Lekbot: a talking and playing robot for children with disabilities. In: Proceedings of the Second Workshop on Speech and Language Processing for Assistive Technologies, pp. 110–119. Association for Computational Linguistics, Stroudsburg (2011). http://dl.acm.org/citation.cfm?id=2140499.2140516
Mazzei, D., Billeci, L., Armato, A., Lazzeri, N., Cisternino, A., Pioggia, G., De Rossi, D.: The FACE of autism. In: Proceedings - IEEE International Workshop on Robot and Human Interactive Communication, pp. 791–796 (2010). https://doi.org/10.1109/ROMAN.2010.5598683
Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G.: Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. BMJ 339 (2009)
Murphy, F.E., Donovan, M., Cunningham, J., Jezequel, T., Garcia, E., Jaeger, A., McCarthy, J., Popovici, E.M.: i4Toys: video technology in toys for improved access to play, entertainment, and education. In: 2015 IEEE International Symposium on Technology and Society (ISTAS), pp. 1–6 (2015)
Pedroso, M.C.S.: A função do brincar para a child com disabilit. Revista Científica da FHO, UNIARARAS 1(2) (2013). http://www.uniararas.br/revistacientifica
Proença, J.P., Quaresma, C., Vieira, P.: New application: adaptation of toys for children with multiple disabilities. Procedia Technol. 17, 351–358 (2014)
Qidwai, U., Shakir, M., Connor, O.B.: Robotic toys for autistic children: innovative tools for teaching and treatment. In: 2013 7th IEEE GCC Conference and Exhibition (GCC) (2013). http://doi.org/10.1109/IEEEGCC.2013.6705773
Ranatunga, I., Balakrishnan, N., Wijayasinghe, I., Popa, D.: User adaptable tasks for differential teaching with applications the robotic autism therapy. In: International Conference on Pervasive Technologies Related to Assistive Environments, pp. 0–6 (2015). https://doi.org/10.1145/2769493.2775129
Schoenherr, N.: Finding educational toys is not hard; key is keeping child’s age in mind. Washington University (2006)
Scott, N., Gabrielli, S.: Archimedes Hawaii: ideal access technology for lifelong learning in the pacific rim. In: CSUN Conference Proceedings (2004)
Soleiman, P., Salehi, S., Mahmoudi, M., Ghavami, M., Moradi, H., Pouretemad, H.: RoboParrot: a robotic platform for human robot interaction, case of autistic children. In: 2014 2nd RSI/ISM International Conference on Robotics and Mechatronics, ICRoM 2014, pp. 711–716 (2014). https://doi.org/10.1109/ICRoM.2014.6990987
Thaller, D., Nussbaum, G.: Accessibility of non-trivial remote controlled models and toys. In: Fourth International Conference on Information and Communication Technology and Accessibility (ICTA) (2013). http://doi.org/10.1109/ICTA.2013.6815314
Vega-Barbas, M., Pau, I., Ferreira, J., Lebis, E., Seoane, F.: Utilizing smart textiles-enabled sensorized toy and playful interactions for assessment of psychomotor development on children. J. Sens. (2015)
Acknowledgments
This research was supported by the Institutional Program of Scholarships for Scientific Initiation of the Federal University of Mato Grosso (UFMT-Brazil) and by the State of Mato Grosso Research Foundation (FAPEMAT-Brazil).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this paper
Cite this paper
dos Santos Nunes, E.P., da Conceição Júnior, V.A., Giraldelli Santos, L.V., Pereira, M.F.L., de Faria Borges, L.C.L. (2017). Inclusive Toys for Rehabilitation of Children with Disability: A Systematic Review. In: Antona, M., Stephanidis, C. (eds) Universal Access in Human–Computer Interaction. Design and Development Approaches and Methods. UAHCI 2017. Lecture Notes in Computer Science(), vol 10277. Springer, Cham. https://doi.org/10.1007/978-3-319-58706-6_41
Download citation
DOI: https://doi.org/10.1007/978-3-319-58706-6_41
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-58705-9
Online ISBN: 978-3-319-58706-6
eBook Packages: Computer ScienceComputer Science (R0)