
Abstract
There are two main aspects of safety and effectiveness in laparoscopic surgery. The first is ensuring an appropriate operation field and maintaining this throughout the procedure. The second is finding the correct tissue plane and applying appropriate traction and counter-traction. To accomplish these requirements, surgeons must know the appropriate pressure to apply to the target organ or tissue. For example, weak operation of the forceps in the left hand during laparoscopic surgery leads to poor visibility owing to a small operational field. Furthermore, poor traction at the point of incision on the dissected plane decreases the dissection efficiency. In contrast, when excessive force is applied, there is an increased risk of organ injury or bleeding from capillary vessels during traction; this is clearly detrimental to the overall safety of the procedure. It is difficult for surgeons to master a feeling for the appropriate pressure to apply. Imitating the techniques of skilled surgeons is essential; however, surgical techniques cannot be imitated on first sight. With the aim of assisting this learning process, we developed Forceps Guiding Correct Operation (FOGCOP), new laparoscopic forceps with sensors. Although they are the same shape as Maryland dissecting forceps, FOGCOP can measure the pressure applied on the shaft of the forceps in three axis directions (X, Y, and Z) and on the jaw. The measured pressures are displayed in real time. Surgeons can insert this device into a 5-mm trocar in the same manner as normal forceps. We conducted experiments to verify the effectiveness of the device. 30 students with no experience of laparoscopic surgery participated in this study. Using a training box, students performed a task to press and pull a rubber plate. We compared the performance of a group of students using FOGCOP (group 1, n = 10) with that of a group using conventional forceps (group 2, n = 10). The results suggest that the feedback provided by FOGCOP may be useful for understanding the force delivered by forceps. To verify the usefulness of the device, FOGCOP was also used in laparoscopic nephrectomy of a pig, a procedure that is part of the training course for laparoscopic surgery. It was possible to dissect a tissue plane in the same manner as with conventional forceps. However, the wire from the sensor sometimes interfered with operation. In future, we intend to upgrade FOGCOP by including a wireless sensor, to improve operability to be closer to that of normal forceps, and to allow this device to be used as an educational tool.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
There was a time when most laparotomies required surgeons to come into direct contact with internal organs and perform operations such as the peeling, ligating, and cutting of tissue. Young surgeons who had little surgical experience participated in surgeries as assistants, thus having many opportunities to come into direct contact with internal organs. Through the resulting accumulation of experience, these young surgeons developed a sensual understanding of the elasticity, firmness, and fragility of each organ, depending on which surgeons learned how to safely and efficiently apply force in surgery.
However, the spread of laparoscopic surgeries since the 2000s has implied a corresponding decrease in opportunities for surgeons to directly come into contact with internal organs and an increased need to understand the elasticity, firmness, and fragility of internal organs using the tactile sense, as conveyed by forceps, and understanding changes in the shape of organs, as seen on monitors during laparoscopic surgeries. Moreover, the use of robots in many types of surgeries has proliferated in recent years, and because robotic surgeries do not involve the use of the tactile sense, it has become extremely difficult to understand the elasticity, firmness, and fragility of internal organs or to learn how to appropriately use force. In addition, surgeons in robotic surgeries manipulate a camera and three arms, performing most of the surgeries alone, which largely does away with opportunities to touch internal organs even where a younger surgeon does participate in a surgery as an assistant.
Although surgical methods have changed, understanding the elasticity, firmness, and fragility of organs, as well as learning the appropriate amount of force to be applied to these organs, is necessary for maintaining the balance between safety and efficiency in surgeries. The knowledge of how to properly apply force ensures a good surgical theater and allows the peeling of tissue with an awareness of plane and proper traction. Accordingly, young surgeons who lack surgical experience must learn to efficiently apply force in laparoscopic surgery.
Learning this, however, is not easy. Even after watching an expert performing a surgery, it can be difficult for an inexperienced surgeon to understand and imitate the application of exactly the same amount of force that the expert applied and that too in the direction the expert did so.
For this reason, we have studied surgical education to aid in understanding organ elasticity and firmness and in learning how to properly use force in laparoscopic surgeries. To assist the study of the elasticity and firmness of organs, we developed an instrument called Pressure Measuring Grasper (PMEG) and reported on its ability to collect data [1].
We have now developed a new device to aid the efficient study of how to apply force in laparoscopic surgeries and call it the forceps guiding correct operation (FOGCOP). In this paper, we introduce the FOGCOP in detail and examine its utility.
2 Materials and Methods
2.1 Device Design
The most basic surgical tool used in laparoscopic surgeries is the Maryland forceps. The open/close function of the forceps is used to grasp and separate tissue. Efficiency is improved as a working space is created through the drawing up and pushing down on tissue and organs, with the addition of traction. Maryland forceps were used as the model of the basic design of FOGCOP, which can measure all of the various forces placed on it on any of the shaft’s axes—X, Y, or Z—as well as the force used to open or close the forceps. Our aim was to display these forces in real time. Through the provision of real-time visibility of the forces on the forceps, young surgeons can analyze their use of force in comparison with that of experts, thereby more quickly acquiring expert skills.
We had three requirements for the creation of these forceps.
Requirement 1: Have the Same Level of Operability as Normal Maryland Forceps to the Extent Possible
Maryland forceps have a variety of tip shapes, and shaft thickness can be 3 mm, 5 mm, or 10 mm. The variety of tip shapes and the different shaft thicknesses can change the way force is applied to the forceps. We designed the shape of the FOGCOP’s tips to be that of the most common type of Maryland forceps, as seen in Fig. 1, and we made the shaft thickness 5 mm. The handle was also designed and fabricated to be similar to that of a standard Maryland forceps. Thus, we were able to ensure the same level of operability for the FOGCOP as that for the standard Maryland forceps and acquired the ability to measure the force used in normal surgical techniques.

Tips of standard Maryland forceps
Requirement 2: To Allow all Forces Applied by the Surgeon to Be Measured
In laparoscopic surgery, surgeons grasp, open, push, and pull and apply other forces in various combinations on the forceps. These forceps must allow the measurement of all the forces that a surgeon may apply on them. Particularly, this means all forces on the X, Y, and Z axes of the shaft, as well as opening and closing forces on the forceps. In addition, in laparoscopic surgeries, the relationship between the force applied to the tips of the forceps and the force of the hand of the surgeon differs according to the depth of the unit. Thus, according to the principle of leverage, the force applied by the surgeon increases at the tips if the forceps are inserted shallowly and decreases as the depth increases (Fig. 2). Expert surgeons can control the force they apply by adjusting the depth of the forceps, thereby operating it safely and efficiently. Inexperienced surgeons must learn this technique of adjusting depth. Because of this, our forceps needed to be able to measure the amount of force applied by the surgeon not only on the tips of the forceps but also on the handle of the forceps.

In laparoscopic surgery, the force applied and force used changes depending on the depth of the part being operated and in accordance with the principle of leverage. A; Operation in shallow section B; Operation in deep section W; Body wall P; Point where shaft meets body wall
Requirement 3: The Forceps Must Be Usable in Animal Laboratories
Current laparoscopic surgery training is done primarily in two ways: through the use of a dry box and by practicing on pigs in animal laboratories. Training in animal laboratories is of course more effective because it is much closer than a dry box to the actual surgical environment. However, opportunities to train in an animal laboratory are extremely rare and limited because of costs and the enforcement of animal rights. We wanted the FOGCOP to be used in animal laboratories to improve the quality of training during these valuable opportunities and for it to be useful in the study of how requisite force can be applied in a short period of time. For these reasons, we felt it necessary to enable the FOGCOP to withstand usage in wet environments, such as those found inside animals.
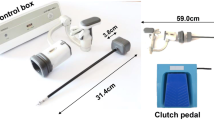
After a trial-and-error process of meeting the above three requirements, we designed the FOGCOP as shown in Fig. 3.

The design of the FOGCOP
The sensors for measuring the amount of force are all in the handle area and are able to measure the force applied on the forceps by the surgeon. By concentrating the sensors in this area, we were able to make the tips and the shaft of the same shape as normal Maryland forceps, enabling the shaft to be inserted into a 5-mm trocar. No sensors are affixed near the tips of the forceps, and because sensors near the handle are covered, the forceps can be used in a wet environment, such as inside the body of an animal.
Codes from the sensor are output to a computer by connecting the forceps to a data logger, thus enabling real-time display of the force used (Fig. 4).

The connection between the FOGCOP and the Data logger
However, the measurement of force is done with a load cell and a very slightly deflected metal, meaning that the amount of deflection is not absolute. The relationship between the amount of force and the amount of deflection of the metal is expected to differ on the basis of various environmental factors, such as temperature and humidity. We made a test bench to calibrate the device by the use of weights each time prior to use. In so doing, we were able to observe the relationship between the amount of deflection and the absolute amount of force.
2.2 Validation Experiments
Validation Experiment 1.
We needed to confirm whether the sensor-equipped FOGCOP that we had made was actually useful for learning “how to apply force to forceps.” There existed the possibility that a validation experiment using people who had experienced or seen laparoscopic surgeries would be biased; hence, we conducted the experiment in cooperation with university students who were not studying medicine. Details of the experiment are as follows:

Using the FOGCOP, a rubber sheet was pushed left and right on the X axis and upward and downward on the Y axis. In the same way, it was pushed and pulled on the Z axis, and was held and spread.
-
(a)
Subjects: 30 university students, none of whom were medical students and none of whom had experience of laparoscopic surgeries. These 30 students were randomly paired into two groups, A and B, numbering 15 each.
-
(b)
Method: A rubber sheet with a slit was affixed within a dry box. Force was applied to the FOGCOP to push the rubber sheet to the right (on the X axis to the right) (Fig. 5). A target level of force was set for this operation. Group A students were shown the amount of force output by the FOGCOP in real time, and they viewed this output as they controlled the amount of force that they were applying so that they could remember the target force level. Conversely, Group B students were not shown the output of the FOGCOP and were asked to adjust the amount of force that they applied on the basis of a target level that was conveyed to them orally; in other words, these students were prompted to “apply more force” if the force that they were using was lower than the target value and to “apply less force” if it was greater. By repeating these instructions, we prompted Group B students to remember the level of target force. Both groups were given one minute to remember the target value using the above methods. A 30-s interval was then provided, after which a test was administered wherein students were asked to apply the target level of force. This same test was also conducted by moving the sheet on the X axis to the left, on the Y axis-upward, and on the Y axis-downward; pushing the sheet on the Z axis; pulling the sheet on the Z axis; and opening and closing the forceps within a 30-s interval, after which the students were again tested for their ability to create the target level of force.
Validation Experiment 2.
We needed to ascertain whether the sensor-equipped FOGCOP was able to measure force in an actual wet environment, such as an animal laboratory, without failure.
We brought the FOGCOP into a training conducted in an actual animal laboratory and had four surgeons use it for a total of one hour. After use, we ascertained, using a test bench, whether the sensors had malfunctioned.
3 Results
3.1 A Subsection Sample
Figure 6(A) shows an overview of the FOGCOP. The forceps tips, shaft, and handle are all similar to those found on normal Maryland forceps although, by locating sensors near the handle, the FOGCOP is able to measure, by using a load cell, the amount of force applied on the shaft on the opening and closing of the forceps. Connecting a data logger for the code output from the sensors allows the graphing and display of forces applied to the X, Y, and Z axes, as well as the opening and closing of the forceps. Graphs are color-coded, and each of the measurements can be displayed simultaneously as well as individually (Fig. 7). As the structure of the handle, as well as the tips, is similar to that found in normal Maryland forceps, the device has a familiar feel when used, which met requirements 1 and 2.

This is an overview of the FOGCOP. Sensors are located near the handle, along with output codes. (B): These are the FOGCOP tips. They are shaped similarly to those on standard Maryland forceps; there is a hole in them through which a thread can be placed though, making provision for weights to be hung on the thread for use in calibration.

Connecting a data logger for the code output from the sensors allows the graphing and display of forces applied to the X, Y, and Z axes, as well as the opening and closing of the forceps. Each forces of the measurements can be displayed simultaneously as well as individually.
Figure 8 shows the calibration of the FOGCOP on a test bench. As can be seen in Fig. 6(B), there is a small hole near the tips of the forceps, through which a thread with a weight attached can be threaded for calibration. The handle is fixed to the test bench, and by hanging various weights from the tips using the thread, we can determine the relationship between force and shaft deflection in that environment.

The calibration of the FOGCOP on a test bench. (A) The FOGCOP is affixed to a test bench, and (B) by hanging various amounts of weights from the tips, we can determine the relationship between force and deflection in that environment.
3.2 Results of Validation Experiments
Validation Experiment 1.
The results of the tests for Groups A and B are shown herein. Figure 9 is a plot of all data, with forces plotted as relative values, and with 1 being the target value. Figure 10 presents a comparison of the groups and shows the differences between the forces applied and the target value. Group A had significantly smaller variances between the forces on the Y axis-upward and downward, Z axis-push and the closing of forceps. This suggests that the group using the FOGCOP was able to learn how to apply force more accurately in a shorter amount of time.

This is a plot of all data, with forces plotted as relative values, and with 1 being the target value. Group A students were shown the amount of force output by the FOGCOP in real time. Group B students were not shown the output of the FOGCOP.

(A) The differences between the forces applied and the target value. This shows the results of X axis and Y axis. (Mann–Whitney U test) (B) The differences between the forces applied and the target value. This shows the results of Z axis and Open-Close. (Mann–Whitney U test)
Validation Experiment 2.
On the day of the experiment, the animal laboratory had a temperature of 26 °C, with a humidity of 67%. Prior to using the FOGCOP, the device was calibrated using a test bench. Over the course of an hour, the FOGCOP was used to peel and open tissues in the body of a pig (Fig. 11). During this time, the tips and shaft of the forceps were continually exposed to blood and fat from the pig; however, a post-use recalibration on the test bench showed no deviations in the measured values from the sensors after use as can be seen in Fig. 11(B). This shows that the FOGCOP met requirement 3.

The usage of the FOGCOP in the animal laboratory
4 Discussion
During surgical operations, the amount of force and the direction in which the force is applied are very important. For example, when applying traction to internal organs using laparoscopic forceps, a force that is excessively strong runs the risk of causing a puncture or rupture to an organ. However, conversely, if the force applied is too weak, with insufficient traction on the organ, the working space may become too small and the efficiency of peeling would be reduced. In addition, depending on the direction of the force, the same level of force may introduce an increased risk of forceps puncture and thus lowered safety. Safe and efficient surgeries require that surgeons learn the proper levels and direction of force (Fig. 12).

Assessment of use on test bench after wet laboratory experiment
Various reports in the past have noted differences between experienced surgeons and beginners in the application of force in laparoscopic surgeries. Yoshida et al. attached 2-centimeter square pressure sensors to the middle of the shaft of Hera forceps and reported differences in the use of force with the forceps, which depended on the skills of surgeons [2]. In addition, Yamanaka et al. discussed sensor-equipped Maryland forceps, and Araki et al. reported on the differences between the gripping forces of experienced and novice surgeons using these same forceps [3, 4].
However, past studies have not reported specifically on how surgeries have improved with a more sensitive application of force or how the application of force can be learned more efficiently, nor have they investigated this issue from the perspective of surgeon training and development [5,6,7]. When an expert surgeon uses a FOGCOP, the complex application of force is made visible and can be analyzed. When a novice surgeon uses the FOGCOP, they can see how they are applying force; hence, the FOGCOP could be very useful as these young surgeons learn how to apply force effectively by studying and imitating expert surgeons in a relatively short period of time.
In validation experiment 1, Group A students were able to more accurately reproduce the level of force required than Group B students. However, we noticed something else from Fig. 9. There is no plot for Group B near the target value 1 for the movement down on the Y axis, push and pull on the Z axis, and so on. This means that almost no one in that group could reproduce the target level of force with oral instructions alone. In an experimental setting, surgical teaching is delivered primarily through oral instruction. We can expect the FOGCOP to be a useful device in the education of surgeons in the future as they learn how to apply force more efficiently.
We must stress once again that it is the surgeon’s application of force that is important here. If hand movements are fine-tuned, everything else is determined by the force on the tips of the forceps in accordance with the principle of leverage. It is important for inexperienced surgeons to understand the hand movements of experts and to learn how to imitate the application of force. For this reason, the next issue to be studied should include the collection and analysis of data from expert surgeons applying force using the FOGCOP.
However, one problem is that the FOGCOP will be used in various environments. The code output from the sensors can interfere with surgical operations, depending on the movements of the surgeon when rotating the forceps. Accordingly, an improved model should be equipped to collect force data wirelessly.
5 Conclusion
We developed new sensor-equipped forceps that can be used like a normal Maryland forceps and that can measure and display all the forces applied on the X, Y, and Z axes and the opening and closing of the forceps. We call this device the forceps guiding correct operation, the acronym for which is FOGCOP. The operation of the forceps is very similar to that of a normal Maryland forceps, and it can be used with a 5-mm trocar. They have a vinyl cover on them that allows them to be used in wet environments, such as animal laboratories. Our study suggests that this device is useful in learning how to apply force more efficiently during surgical procedures. We propose that this device be used in surgical education to enable not only researchers and inexperienced doctors to learn the proper application of force but also medical students, who can also use it in practice and experience the joy and difficulty of laparoscopic surgery.
References
Sawada, A., Kume, N., et al.: Development of a novel tool for assessing deformation and hardness of real organs: Pressure Measuring Grasper (PMEG). Adv. Biomed. Eng. 5, 68–75 (2016)
Yoshida, K., Kinoshita, H., et al.: Analysis of laparoscopic dissection skill by instrument tip force measurement. Surg. Endosc. 27(6), 2193–2200 (2013)
Yamanaka, H., Makiyama, K., et al.: Measurement of the physical properties during laparoscopic surgery performed on pigs by using forceps with pressure sensors. Adv. Urol. 2015, Article ID 495308, 10 pages (2015)
Araki, A., Makiyama, K., et al.: Comparison of the performance of experienced and novice surgeons: measurement of gripping force during laparoscopic surgery performed on pigs using forceps with pressure sensors. Surg. Endosc. 31(4), 1999–2005 (2017)
Puangmali, P., Althoefer, K., et al.: State-of-the-art in force and tactile sensing for minimally invasive surgery. IEEE Sens. J. 8(4), 371–381 (2008)
Trejos, A.L., Patel, R.V., et al.: A sensorized instrument for skills assessment and training in minimally invasive surgery. J. Med. Devices 3(4), 041002 (2009)
Ly, H.H., et al.: Grasper having tactile sensing function using acoustic reflection for laparoscopic surgery. Int. J. CARS 12(8), 1333–1343 (2017)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Sawada, A. et al. (2018). Laparoscopic Forceps with Force Feedback. In: Kurosu, M. (eds) Human-Computer Interaction. Interaction in Context. HCI 2018. Lecture Notes in Computer Science(), vol 10902. Springer, Cham. https://doi.org/10.1007/978-3-319-91244-8_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-91244-8_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-91243-1
Online ISBN: 978-3-319-91244-8
eBook Packages: Computer ScienceComputer Science (R0)