
Abstract
Despite the recent increase in research and development of mobile self-care tools, there are very few solutions regarding the prevention of negative health effects of menopause. Moreover, most of these solutions are not based on well-founded user models, such as personas, and fail to seize the potential of persuasive mobile technology, which results in a user experience that is neither engaging nor adaptive. In this paper, we describe how we designed personas during the development of a mobile application for menopause self-care. For this design, we used the principles of the Persuasive Systems Design model and the Just-in-Time Adaptive Interventions framework, along with participatory techniques and demographic data analysis. This approach is not limited to menopause, as it could be used to reliably represent users in the interaction design of mobile self-care solutions in other health-related domains.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others



Keywords
1 Introduction
The world population is aging rapidly, especially in the most economically developed countries. This demographic shift implies significant changes at the societal and economic levels, and has already begun to have a negative impact on public healthcare systems. For these reasons, there has been increasing interest in healthy aging and personal self-care, particularly by means of innovative Information and Communication Technology (ICT). The plethora of available health and fitness smartphone applications (apps), as well as related research initiatives, are a prime example of this phenomenon. However, most of these apps are merely trackers that do not adapt to users’ health status and behavior, and many do not apply best practices to human-computer interaction (HCI), with both factors leading to poor user adherence. These issues are particularly true for the few available apps for women that focus on menopause and its effects.
Menopause is a natural and inevitable part of women’s aging, involving the loss of the body’s reproductive function and significant hormonal changes during the menopausal transition. In turn, women’s health-related quality of life changes during this transition, often in relation to the absence or presence of symptoms [1]. Although each woman’s experience varies widely, these symptoms include hot flashes and night sweats, urogenital atrophy, sexual dysfunction, mood changes, bone loss, and a predisposition to diabetes and cardiovascular disease [2]. However, many women ignore such changes and risks, and do not realize the need to improve their health-related behavior and lifestyle to reduce the negative effects of menopause. Inspired by the increasing prevalence of smartphones across the general population, we think that an adaptive and personalized app that empowers women regarding their menopausal transition would greatly aid in self-care. This is the main rationale behind the ongoing project Vita Nova.
Vita Nova involves the development of a mobile app and service to accompany and coach women regarding menopause, automatically adapting to their wants and needs in order to induce positive health-related behavioral changes. The main goal of the service is to reduce the higher cardiovascular risk inherent in the menopausal transition. A multidisciplinary consortium in the Tuscany Region (Italy) is currently carrying out the project. This consortium is composed of members with different backgrounds and expertise: three private companies (business and ICT services), a public research organization (data modelling and HCI research), a public university (women-related bio-clinical and socioeconomics research), and an external consultant (psychology). From the beginning the consortium decided to utilize a user-centered design, in order to overcome many of the aforementioned HCI issues of user adherence in health-related apps. However, we soon realized that research on interaction design of health-related apps for our target users (women in pre-menopause and menopause) was almost non-existent. As a result, we had little information and few guidelines on which to base the persona method in order to better define and communicate certain aspects of the project (e.g., the app’s core features and interaction flows). In light of this, we decided to take advantage of the research we were already doing regarding women’s health status and behavior, health-related persuasion, and self-care through mobile technology, in order to create such personas, as detailed in the following sections.
2 Background
2.1 Self-Care Through Mobile Health Solutions
By self-care, we refer to the activities people perform in order to prevent their own disease, limit their own illness, and promote and restore their own health, without professional aid but relying on skills and knowledge derived from both lay and professional experience [3]. Health promotion has traditionally been the domain of healthcare professionals, but recent advances in ICT, the ever-increasing burden of healthcare systems, and the ideology of patient empowerment have led to a shift toward personal self-care. In particular, the spread of pervasive and ubiquitous computing (e.g., smartphones, wearable devices, domestic sensors) has spurred the development of mobile health technology and solutions (also known as m-Health) for self-care. Nonetheless, the availability of m-Health self-care solutions specifically targeting women in menopause, as well as the respective scientific literature, are very limited. Moreover, most of these solutions only offer tracking of diet and symptoms, and general information about menopause, or they are used in very narrow clinical contexts. Among the few available apps present in the scientific literature we find MenoPro, conceived and designed for iOS and Android by the North American Menopause Society [4]. MenoPro has the goal of helping gynecology clinicians decide whether patients should undertake pharmacological treatment for menopausal symptoms. MenoPro is intended to be used not only by clinicians, but also by women, as it offers a patient mode. However, this mode has very limited features, as it does not offer self-monitoring over time, is restricted to women aged over 45 years, and does not take into consideration behavioral changes. Furthermore, the available research related to this app does not seem to take into account design aspects of human-computer interaction.
In fact, we found only one study that specifically focuses on the HCI aspect of designing apps for women in menopause [5]. This study investigated the needs of middle-aged Korean women for a menopause-related app, using focus group interviews. The main features of the app envisioned were menstrual tracking and social network support. Given that this study was on the early stages of the app’s development cycle, there is no information regarding interaction mechanisms and workflow, nor references to a particular behavior change theory. The study concluded that such an app should be simple and validated by healthcare professionals, and it should provide personalized suggestions, means for social support (family and friends), and comprehensible tracking and data visualization tools. These results are in line with a study on the quality of health and fitness apps in general [6], which identified the fundamental features that such apps should have: user-friendly interfaces, low learning curve, reliable, real-time personalized feed-back, user customization, incorporation of evidence-based behavior change techniques, involvement of health professionals, and social networking support. Incidentally, all of these characteristics are closely related to the more general design of effective persuasive technology.
2.2 Persuasive Systems
Since time immemorial people have tried to learn how to persuade other people to do or believe something. For instance, already in ancient Greece Aristotle identified three fundamental kinds of persuasive appeal: ethos, appeal to ethics, based on the credibility of the persuader; pathos, appeal to emotion, based on creating an emotional response; and logos, an appeal to logic, based on reason. Interestingly, these and other principles of rhetoric described by Aristotle and later scholars can also be applied to computer systems that act as persuaders, as stated by Fogg [7], the pioneer of persuasive systems. Fogg proposed the use of computers as persuasive technologies, a field of study that he called captology, based on the acronym of the subject matter [8]. Although the term captology has fallen into disuse [9], Fogg’s work paved the way to more recent and detailed conceptual models for persuasive technology, such as the Persuasive Systems Design (PSD) model. PSD was developed by Oinas-Kukkonen and Harjumaa to design and evaluate persuasive systems, as well as to describe their content and software functionality [10]. In the context of PSD, the authors build upon their prior definition of persuasive systems as “computerized software or information systems designed to reinforce, change or shape attitudes or behaviors or both without using coercion or deception” [11]. Accordingly, PSD derives its principles from psychology and rhetoric, adapting them to the intersection of four key computer-based fields: human-computer interaction, computer-mediated communication, information systems, and affective computing [12]. The PSD conceptual model (see Fig. 1) is divided into two main aspects: persuasion context and design principles. The persuasion context is composed of three elements that influence whether persuasion can take place or not: intent, event, and strategy. The design principles of the PSD model focus on the system’s operational level of persuasion and are divided into four dimensions: primary task support, dialogue support, system credibility support, and social support. For a more detailed description of both aspects see [10].

Overview of the PSD conceptual model
It should be noted that PSD is a general model that can be used across heterogeneous domains such as education and learning [13], ecological consumption [14], marketing and commerce [15], as well as public security and safety [16]. Nonetheless, the health-related domain is the most prevalent area in which PSD is used. For instance, a 2014 review [9] on the efficacy of persuasive technology in 95 studies (in 89 papers), reported that 47.4% of them were related to a health and/or exercise setting, among which several were based on the PSD model. Incidentally, the review’s authors concluded that “persuasive technologies indeed seem to persuade people into various behaviors” [9], with one decisive aspect being whether the user is trying to accomplish the target change with or without the system. For health-related initiatives this aspect is less of a problem, as people usually want to improve their own health status regardless of the use technology. Furthermore, the use of PSD has been shown to have positive effects on adherence to health-related persuasive systems that are remotely accessible, such as web-based interventions [17]. For these reasons, we deem PSD particularly apt as the underlying model for persuasive self-care applications, but we think that it is not specific enough to deliver health-related behavior interventions via mobile technology.
2.3 Just-in-Time Adaptive Interventions
Health-related behavior interventions (henceforth interventions) are efforts that promote behavioral changes to improve a person’s health status and reduce potential risk factors. Therefore, an intervention can be seen as a specialized kind of persuasion regarding health behavior. An adaptive intervention is “a sequence of decision rules that specify how intervention options should be adapted to an individual’s characteristics and changing needs, with the general aim to optimize the long-term effectiveness of the intervention” [18]. Expanding on this concept and based on the existing research on mobile health apps, around 2014 the framework just-in-time adaptive interventions (JITAI) emerged. A solution based on JITAI aims to “provide information, nudges, and interventions when needed or appropriate, tailored to the individual’s needs and context, via mobile technologies” [19]. The JITAI framework is composed of four key components common to any adaptive intervention: decision points, intervention options, tailoring variables, and decision rules. The following are descriptions adapted from [20] of how these components are employed in the context of JITAI.
-
Decision points are points in time at which decisions regarding treatment must be made. In JITAI their selection and frequency are flexible, and they can be classified as scientist-specified or participant-initiated.
-
Intervention options include the types of support (instrumental, emotional), sources of support (automated, professional, peer group), and modes of support delivery (support provision and/or support availability). In the continuum of health proximal-distal outcomes, intervention options that target proximal outcomes are crucial, especially in the case of heightened user vulnerability.
-
Tailoring variables are specific pieces of information concerning the user that are used to make treatment decisions. These variables can be gathered through active assessments, passive assessments, or both.
-
Decision rules operationalize individualization by specifying which intervention option to offer, to whom, and when (Fig. 2), according to the values of tailoring variables. They systematically connect tailoring variables (along with their levels, thresholds and ranges) with intervention options, in the form of if-then statements.
Fig. 2. 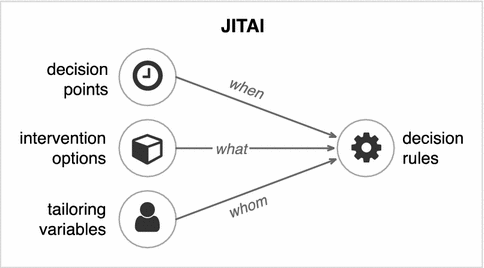
Main components of the JITAI framework

The JITAI framework is a promising reference methodology for developing not only smartphone health and fitness apps, but also solutions for other ubiquitous and pervasive computing technologies. Despite being relatively new, JITAI has already been proposed or used to develop solutions for depression and anxiety [21], to reduce sedentariness [22], and, in particular, to treat addictive behavior [23], including quitting smoking [24]. However, there are some open questions regarding best practices for design and implementation of JITAI, such as the use of micro-randomized trials [25]. Nonetheless, we think that JITAI, together with PSD, could also be used to improve the interaction design process of a persuasive and adaptive mobile health app, particularly in the definition of personas.
2.4 Persona Use in Product Design
Personas, or user models, “are detailed, composite user archetypes that represent distinct groupings of behaviors, attitudes, aptitudes, goals, and motivations” [26]. They were introduced in 1998 by Alan Cooper as a support method for interaction design [27]. The key idea behind the method is that “the best way to successfully accommodate a variety of users is to design for specific types of individuals with specific needs” [26], and that personas represent those users with the larger set of key characteristics. Thus, personas help designers determine what a product is and its behavior, communicate with project’s stakeholders, build consensus and commitment around the product design, measure the design’s effectiveness, and contribute to other project efforts (e.g., marketing and sales).
Personas mainly describe the context of people’s behavior regarding a certain product—behavior that is primarily motivated by people’s goals. Thus, goals should guide the design of a product’s functions and the tasks with which people attain them. To better characterize people’s goals in product design, we can refer to the three-leveled theory of cognitive and emotional processing, introduced by Norman [28]. Its design levels, in increasing order, are: (1) visceral, the intuitive reaction to a product’s sensory aspects (e.g., visual, touch, aural) that are perceived prior to significant interaction; (2) behavioral (simple daily behaviors), which can enhance or inhibit both visceral reactions and reflective responses and has been the main focus of traditional design; (3) reflective, which involves reflection and careful thought on past experiences, and can enhance or inhibit behavioral processing, yet does not affect visceral reactions. Each level has a different timeframe (the shorter the more immediate) and degree of consciousness (the higher the more conscious), and implies different design considerations. Based this theory, in interaction design and to better define personas, we could delineate three types of user goals [26]:
-
Experience goals: how the user wants to feel (visceral level). They provide focus for a product’s sensorial characteristics: visual design, physical design, interactive feel (latency, transitions, etc.).
-
End goals: what the user wants to do (behavioral level). They represent user task motivation, linked to a given product, which should be satisfied.
-
Life goals: who the user wants to be (reflective level). They denote users’ personal aspirations and explain the reasons behind wanting to accomplish their end goals.
Therefore, personas could help m-Health designers identify user goals and the desired features on which to focus. For instance, the use of personas was a valuable methodological approach in the design of a tool for older Chinese people with diabetes [29], in which authors focused on three main aspects to model user behavior and characteristics: technical (e.g., attitudes, skills), demographics, and health specifics (e.g., diagnosis, practices). A more recent example is the Consumer Navigation of Electronic Cardiovascular Tools (CONNECT), a web-based desktop and mobile application integrated with the user’s primary care electronic health record, which also made great use of the PSD model [30]. In the initial phase of the project, four personas were developed to better define the target audience and needs of older people with high risk of cardiovascular disease. The personas’ definition included information such as cardiovascular risk, occupation, household composition, ethnicity, as well as the persona’s story, needs, health motivations, influencers, opportunities, frustrations, and relationship with healthcare providers and to technology. Then, the designers specified the persuasion context and design principles of CONNECT according to the PSD model.
For this reason, our persona design process expands this approach by taking into consideration not only the PSD model but also the JITAI framework, to better define user goals and attributes in the context of m-Health for self-care.
3 Persona Design Process
In order to define the personas for Vita Nova, we first conducted initial participatory user research, with both consortium stakeholders and a sample of target users; later we defined the features and principles that the service should have based on the PSD model; and finally, we conducted an expert consultation and demographic analysis to define the initial set of tailoring variables for JITAI. These steps are detailed below.
3.1 Initial Participatory User Research
Although there are several approaches to persona design, prior to their description there should always be extensive user research and analysis, typically carried out by gathering data obtained from a combination of user interviews, internal discussions, and direct observation [31]. It should be noted that Cooper’s original interaction design process does not consider personas as part of a participatory approach. In PD, actual (or potential) users are involved along the design process, whereas personas are models intentionally built based on aggregated data collected from actual (or potential) users. Nonetheless, the use of personas in PD has been proven useful for scenario design and product development in general [32], since they share common data gathering techniques. Accordingly, we used a set of PD practices for moderate group sizes (up to 40 participants) and in the phases of the project, midway between the design activities and the user world, based on the taxonomy of Muller and Kuhn for PD practices [33]. In our case, we had already started with a participatory design (PD) approach, involving both the project consortium members and potential end users of the app, to better define the consortium’s vision according to their comments [34].
First, we held semi-structured workshops with members of the consortium to consolidate a common vision of the app and a set of expected core functionalities. We then conducted focus group interviews (FGI) with 26 potential users, all women aged 48 to 69 years, to understand their wants and needs, and to gather qualitative feedback on the consortium’s vision of the app. Based on this feedback the consortium decided to use storyboard prototyping and conduct a questionnaire to refine the app’s core features with an available subset of the FGI participants (18 this time). The storyboards depicted five main use case scenarios to describe how a user would interact with the app and vice versa. As the storyboards’ protagonist we used a provisional persona called Laura, a persona not based upon detailed qualitative data [26], which acted as a rhetorical tool to communicate the consortium’s assumptions about the target users and the initial vision of app’s main features. Laura is a 50-year-old woman; she is a low-rate daily smoker, performs moderate physical activity, frequently eats unhealthy food, has a moderate body mass index (BMI), and works in an office environment. Laura would like to achieve and maintain a healthier weight, which is why she bought a wearable fitness tracker to monitor her progress while walking briskly. However, she has already begun the menopause transition and is suffering its effects, especially frequent hot flashes. For these reasons, she is interested in an app to better manage her symptoms during menopause and attain a better health-related quality of life.
As a result of this initial approach, we gathered valuable data from the participants regarding smartphone and wearable device use, personal health behavior and tracking habits, interest in the app, and desired functionalities, content, and interaction flows, as well as disposition of and concerns about personal information. These data in turn allowed us to narrow the experience, end, and life goals of our personas. In our case, the primary life goal of users is to attain and maintain a good health-related quality of life during and after menopause. To achieve this, participants wanted the flexibility to focus on as few or many end goals as desired, such as symptom monitoring, diet improvement, physical activity increase, etc. And because of the utmost importance given to their health, participants’ experience goals primarily focus on understandable content, professional-looking but friendly appearance, app’s credibility and validity, responsive interface, and reassurance in terms of security and privacy. Accordingly, we decided to focus on six user aspects, which we grouped into two sets (see Fig. 3). The first set, health status and behavior (bio-clinical condition, vital statistics and lifestyle, and psychological traits and condition), is the basis of the persuasion context. The second set, user interaction features (skills and knowledge, service expectations, and health goals), is the basis of the interaction design principles.

Main aspects of Vita Nova’s personas
3.2 Selection of PSD Features and Principles
Based on the outcomes of our participatory user research and on the PSD model heuristic described in [12], we outlined the persuasion context and the design principles for our system as follows.
Persuasion Context
-
Intent. The system aims to persuade Italian women to adopt and maintain good health-related behaviors before, during, and after the menopausal transition, as well as to inform them about menopause (i.e., both behavior and attitude changes). The persuader is a multidisciplinary consortium of private and public organizations (detailed in the Introduction), which aims to improve the health-related quality of life of women in menopause, opening as a result new research and commercial opportunities.
-
Event. The use context is about personalized, adaptive and automatic self-care for women in menopause, with the menopausal transition usually starting around ages 45–60 years, although we also target women in early menopause. We revised the age of target users compared to our initial FGI based on the feedback of our health experts, taking into account the preventative scope of Vita Nova. The user context of the system regards women who are interested and willing to reduce menopausal effects and improve their health in a simple and independent manner via innovative mobile technologies. The use of the latter is the basis of the technology context: an online mobile application that is primarily single-user, but with a few multi-user features (e.g., to allow peer support).
-
Strategy. The message will be primarily in the form of a tracking and assistive health tool. The type of content will be informational (general tips, personalized suggestions) and stimulant (alarms, reminders, action prompts). The kind of appeal will be a mix between logos, pathos, and ethos, which will be adapted to the user based on the principles of the JITAI framework. The route will be indirect, with the several available arguments being tailored to the user.
Design Principles
-
Primary task support. We will use reduction (simplifying the information available to users, with the possibility of more detailed information if needed), tailoring and personalization (based on JITAI), self-monitoring (e.g., diet, symptoms, physical activity, humor), and simulation.
-
Dialogue support. We will use praise, reminders, suggestions (both general and personalized), similarity and liking (necessary to appeal to users’ visceral level of cognitive functioning and satisfy their experience goals).
-
System credibility support. Besides aiming at a professional and simple look-and-feel (surface credibility) based Google’s Material Design guidelines, we will provide validated suggestions and information, based on the experience and knowledge of our health-related experts (trustworthiness, expertise, authority, verifiability), as well as providing the necessary contact means for the consortium’s representatives (real-world feel).
-
Social support. At the moment, we will focus primarily on the use of recognition, cooperation, and competition as a means of interacting with other persons.
3.3 Tailoring Variables for Women’s Health Status and Behavior
Regarding the JITAI framework, we had already started to work on tailoring variables to model women’s health status and behavior in pre-menopause and menopause, before realizing that such variables could be influenced by the persona definition, and at the same time these variables could influence the personas. Therefore, we had also adjusted the persona design, and will continue to do so if necessary, taking into account the tailoring variables and vice versa, as well as the project’s persuasion context and design principles. To define these variables, the user modelling team, together with the health-related experts, made use of their experience and knowledge of the domain, as well as the state-of-the-art literature. In many variable definitions, we also have made use of data analyses and reports on women’s health and socio-economics from the Italian National Institute for Statistics (ISTAT).
At the moment of writing, an initial set of 75 tailoring variables have already been defined. Most of these variables (49) come from the bio-clinical domain (e.g., menopause age onset, smoking, physical activity level, weekly salt consumption, frequency of menopausal symptoms); 16 from the socio-economic domain (e.g., marital status, income level, employment status); and 10 from the psychological domain (e.g., willingness to change, locus of control, appeals). To verify the applicability of these variables and their related wording (e.g., clarity, willingness to respond), we also carried out a questionnaire among potential users. This questionnaire was filled out by 43 participants recruited in the Tuscany region, on a voluntary basis, among a population of women in menopause and pre-menopause who were free of chronic diseases. However, given the sensitive nature of the collected data and based on the aforementioned preventative scope of Vita Nova, once we had the participants’ answers we further excluded nine women with a BMI less than 18.5 (underweight) or more than 30 (obesity), or not aged 40–60 years, leaving 34 participants who corresponded to our target users.
Thanks to this questionnaire we were able to refine our JITAI tailoring variables where needed, and we also gathered valuable information for the definition of our personas. For instance, of the aforementioned 34 participants, 15 declared themselves to be in menopause, and one was unsure about it. The average BMI of these participants was 22.1 (s = 2.8). Regarding smoking, eight of them are smokers, with an average of 8.8 cigarettes a day (s = 3.1), and two of them were former smokers. All of those who were smokers declared being rather insecure regarding their control over smoking. With regard to physical activity, the average minutes a week of moderate physical activity were 158.5 (s = 197), and 34.2 min a week (s = 74) of intense physical activity. Concerning the perceived inconvenience of symptoms related to menopause, the five most important symptoms (ordered from more to less inconvenient) were tiredness, mood changes, lack of energy, musculoskeletal pain, and loss of concentration.
As our JITAI components’ definition continues to evolve we also expect to update our persona description in order to maintain a dynamic yet consistent user representation. In particular, once Vita Nova has attained a reliable user base, these data could also be complemented with historic data on users’ behavior or demographics.
3.4 Vita Nova’s Personas
Based on the qualitative and quantitative data of the participatory user research and our variable questionnaire, we proceeded to map participants’ behavioral variables to identify eventual patterns. For this, we used a relative linear mapping approach, as suggested by Cooper [26], in which we could visually identify clusters of participants along a behavioral axis, as illustrated in Fig. 4. Then, on the basis of the previously identified PSD principles and features, and taking into account the tailoring variables of JITAI, we selected the personas’ main attributes that cover our six aspects of interest (Fig. 3). Finally, based on these attributes and behavior patterns, we created four personas: Anna, a 52-year-old housewife in perimenopause; Elena, a 48-year-old office worker in menopause; Beatrice, a 58-year-old retiree approaching post-menopause; and Carla, a 44-year-old bank clerk in early menopause. Anna is the primary persona, i.e., she is the main target of our design. Elena, Beatrice, and Carla are secondary personas. In addition, in order to better communicate with the project stakeholders, we created an overview format in which each persona could be succinctly described. For instance, Fig. 5 represents the overview of Anna.

Example of participants’ behavioral mapping

Overview of Anna, the primary persona of Vita Nova
In this overview, from top left to bottom right, we can quickly understand the persona’s main motivation (using a representative quote), her vital statistics and socio-economic situation, her personality (using qualitative scales), her current menopause phase status (from perimenopause to post-menopause), the most effective appeals to persuade her (using Aristotle’s rhetoric triangle), what her main goals are (at the visceral, behavioral, and reflective levels), her technological context in regards to smartphone use, as well as her menopause-related behavior (via key indicators ranging from negative to positive) and condition (indicating the inconvenience level caused by the main menopause symptoms).
To depict our personas, we decided to use photos instead of drawings or no picture at all, as it gives the personas a heightened sense of realism and effectiveness [35]. However, it should be noted that in some instances the use of photos may not be desirable because it could alienate some individuals, such as in the case of products for an international or global market [31]. The personas’ photos were derived from the Exactitudes series, by photographer Versluis and profiler Uyttenbroek, a project that has documented numerous identities in major European cities for the past 20 years. Because these derivations are only for research purposes, they fall under fair use as well as the limitations and exceptions to copyright.
Given that our personas are reliable representations of women in different stages of life and phases of menopause, each with different needs and wants, the consortium is confident in utilizing them during the rest of the project. Still, as previously mentioned, our personas’ definition will not be static. We will continue to refine our personas’ definition as Vita Nova continues, based on future PSD persuasion principles that we adopt, the evolution of JITAI tailoring variables, and on the feedback of real users. We believe that keeping personas “alive” and updated is an important goal that designers should pursue, as these not only help in guiding the interaction design process of a product, but also because they are a valuable tool to communicate with the project stakeholders, users, and other people external to the project.
4 Conclusion
We have presented the principles of persuasive systems and just-in-time adaptive interventions, and how we used them to define personas during the interaction design process of a menopause self-care app. This approach allowed us to come up with reliable representations of our target users and their goals, which in turn enables us to better delimit and communicate our project’s scope and features. Moreover, such an approach is not limited to the menopause domain, as it could be also applied to other self-care apps in other health-related domains, especially to define user goals, which is, in our opinion, the most challenging and important aspect of this process. Obviously, the main life goal of users of health-related apps is to be healthy. However, the linked life, end, and experience goals are not necessarily the same across health-related domains or individuals. For instance, on the one hand, users of apps for chronic conditions may also have as a life goal to be more autonomous and to lessen their caregivers’ burden. On the other hand, users of fitness apps may also have as a life goal to be more attractive and popular, as staying fit is a status symbol. By the same token, a chronic patient may prefer a simple and reliable device regardless of its aesthetics (experience goal) to ensure daily pill intake (end goal); while a fitness user may desire a stylish and elegant wearable device (experience goal) to monitor and improve workout performance (end goal). Finally, we hope that our research inspires future studies regarding mobile self-care solutions focused on women’s health.
References
Avis, N.E., et al.: Change in health-related quality of life over the menopausal transition in a multiethnic cohort of middle-aged women. In: Study of Women’s Health Across the Nation (SWAN), Menopause (New York, NY), vol. 16, no. 5, p. 860 (2009)
Davis, S.R., et al.: Menopause. Nat. Rev. Disease Prim. 1, 15054 (2015)
Levin, L.S., Idler, E.L.: Self-care in health. Annu. Rev. Publ. Health 4(1), 181–201 (1983)
Manson, J.E., et al.: Algorithm and mobile app for menopausal symptom management and hormonal/non-hormonal therapy decision making: a clinical decision-support tool from The North American Menopause Society. Menopause 22(3), 247–253 (2015)
Lee, M., et al.: Understanding women’s needs in menopause for development of mHealth. In: Proceedings of 2015 Workshop on Pervasive Wireless Healthcare. ACM (2015)
Higgins, J.P.: Smartphone applications for patients’ health and fitness. Am. J. Med. 129(1), 11–19 (2016)
Fogg, B.J.: Persuasive computers: perspectives and research directions. In: Proceedings of SIGCHI Conference on Human Factors in Computing Systems. ACM Press/Addison-Wesley Publishing Co. (1998)
Fogg, B.: Captology: the study of computers as persuasive technologies. In: CHI 1997 Extended Abstracts on Human Factors in Computing Systems. ACM (1997)
Hamari, J., Koivisto, J., Pakkanen, T.: Do persuasive technologies persuade? - a review of empirical studies. In: Spagnolli, A., Chittaro, L., Gamberini, L. (eds.) PERSUASIVE 2014. LNCS, vol. 8462, pp. 118–136. Springer, Cham (2014). https://doi.org/10.1007/978-3-319-07127-5_11
Oinas-Kukkonen, H., Harjumaa, M.: Persuasive systems design: key issues, process model, and system features. Commun. Assoc. Inf. Syst. 24(1), 28 (2009)
Oinas-Kukkonen, H., Harjumaa, M.: Towards deeper understanding of persuasion in software and information systems. In: First International Conference on Advances in Computer-Human Interaction. IEEE (2008)
Torning, K., Oinas-Kukkonen, H.: Persuasive system design: state of the art and future directions. In: Proceedings of 4th International Conference on Persuasive Technology. ACM (2009)
Ashaikh, R.A., Wilson, S., Jones, S.: A persuasive social actor for activity awareness in learning groups. In: Proceedings of 30th International BCS Human Computer Interaction Conference: Fusion! BCS Learning & Development Ltd. (2016)
Shevchuk, N., Oinas-Kukkonen, H.: Exploring green information systems and technologies as persuasive systems: a systematic review of applications in published research (2016)
Alhammad, M.M., Gulliver, S.R.: Online persuasion for e-commerce websites. In: Proceedings of 28th International BCS Human Computer Interaction Conference on HCI 2014-Sand, Sea and Sky-Holiday HCI. BCS (2014)
Kotthaus, C., Ludwig, T., Pipek, V.: Persuasive system design analysis of mobile warning apps for citizens (2011)
Kelders, S.M., et al.: Persuasive system design does matter: a systematic review of adherence to web-based interventions. J. Med. Internet Res. 14(6), 2–25 (2012)
Nahum-Shani, I., et al.: Experimental design and primary data analysis methods for comparing adaptive interventions. Psychol. Methods 17(4), 457 (2012)
Spruijt-Metz, D., Nilsen, W.: Dynamic models of behavior for just-in-time adaptive interventions. IEEE Pervasive Comput. 13(3), 13–17 (2014)
Nahum-Shani, I., et al.: Just in time adaptive interventions (JITAIs): an organizing framework for ongoing health behavior support. Methodology Center Technical report (14-126) (2014)
Schueller, S.M., Aguilera, A., Mohr, D.C.: Ecological momentary interventions for depression and anxiety. Depress. Anxiety 34, 540–545 (2017)
Thomas, J.G., Bond, D.S.: Behavioral response to a just-in-time adaptive intervention (JITAI) to reduce sedentary behavior in obese adults: implications for JITAI optimization. Health Psychol. 34(S), 1261 (2015)
Goldstein, S.P., et al.: Return of the JITAI: applying a just-in-time adaptive intervention framework to the development of m-Health solutions for addictive behaviors. Int. J. Behav. Med. 24, 673–682 (2017)
Naughton, F.: Delivering “Just-In-Time” smoking cessation support via mobile phones: current knowledge and future directions. Nicotine Tob. Res. 19(3), 379–383 (2017)
Klasnja, P., et al.: Microrandomized trials: an experimental design for developing just-in-time adaptive interventions. Health Psychol. 34(1), 1220 (2015)
Cooper, A., Reimann, R., Cronin, D.: About Face 3: The Essentials of Interaction Design. Wiley, New York (2007)
Cooper, A.: The Inmates are Running the Asylum-Why High-Tech Products Drive Us Crazy and How 2 to Restore the Sanity. SAMS, Carmel (1999). ISBN 0-67231-649-8
Norman, D.: Emotional Design. Basic Books, New York (2005)
LeRouge, C., et al.: User profiles and personas in the design and development of consumer health technologies. Int. J. Med. Inform. 82(11), e251–e268 (2013)
Neubeck, L., et al.: Development of an integrated e-health tool for people with, or at high risk of, cardiovascular disease: The Consumer Navigation of Electronic Cardiovascular Tools (CONNECT) web application. Int. J. Med. Inform. 96, 24–37 (2016)
Nielsen, L., et al.: A template for design personas: analysis of 47 persona descriptions from danish industries and organizations. Int. J. Sociotechnol. Knowl. Dev. (IJSKD) 7(1), 45–61 (2015)
Grudin, J., Pruitt, J.: Personas, participatory design and product development: an infrastructure for engagement. In: PDC (2002)
Muller, M.J., Kuhn, S.: Participatory design. Commun. ACM 36(6), 24–28 (1993)
Trujillo, A., Buzzi, M.C.: Participatory user requirements elicitation for personal menopause app. In: Proceedings of 9th Nordic Conference on Human-Computer Interaction. ACM (2016)
Giboin, A.: From individual to collective personas modeling realistic groups and communities of users (and not only realistic individual users). In: Fourth International Conference on Advances in Computer-Human Interaction (ACHI 2011) (2011)
Acknowledgements
This work was supported by the Vita Nova project (CUP CIPE D18C15000130008), funded by the Tuscany Region and the Italian Ministry of Education, Universities and Research (MIUR), as part of the PAR FAS (now FSC) and FAR programs. We would also like to express our gratitude to Giulia Mascagni and Andrea Giannini of the University of Pisa for their contribution in the definition of the tailoring variables, as well as for their help in organizing and recruiting participants for our focus group interviews and questionnaires.

Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Trujillo, A., Senette, C., Buzzi, M.C. (2018). Persona Design for Just-in-Time Adaptive and Persuasive Interfaces in Menopause Self-care. In: Marcus, A., Wang, W. (eds) Design, User Experience, and Usability: Users, Contexts and Case Studies. DUXU 2018. Lecture Notes in Computer Science(), vol 10920. Springer, Cham. https://doi.org/10.1007/978-3-319-91806-8_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-91806-8_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-91805-1
Online ISBN: 978-3-319-91806-8
eBook Packages: Computer ScienceComputer Science (R0)