
Abstract
Research on degenerative spondylolisthesis (DS) has focused primarily on the biomechanical responses of pathological segments, with few studies involving muscle modelling in simulated analysis, leading to an emphasis on the back muscles in physical therapy, neglecting the ventral muscles. The purpose of this study was to quantitatively analyse the biomechanical response of the spinopelvic complex and surrounding muscle groups in DS patients using integrative modelling. The findings may aid in the development of more comprehensive rehabilitation strategies for DS patients. Two new finite element spinopelvic complex models with detailed muscles for normal spine and DS spine (L4 forwards slippage) modelling were established and validated at multiple levels. Then, the spinopelvic position parameters including peak stress of the lumbar isthmic-cortical bone, intervertebral discs, and facet joints; peak strain of the ligaments; peak force of the muscles; and percentage difference in the range of motion were analysed and compared under flexion–extension (F-E), lateral bending (LB), and axial rotation (AR) loading conditions between the two models. Compared with the normal spine model, the DS spine model exhibited greater stress and strain in adjacent biological tissues. Stress at the L4/5 disc and facet joints under AR and LB conditions was approximately 6.6 times greater in the DS spine model than in the normal model, the posterior longitudinal ligament peak strain in the normal model was 1/10 of that in the DS model, and more high-stress areas were found in the DS model, with stress notably transferring forwards. Additionally, compared with the normal spine model, the DS model exhibited greater muscle tensile forces in the lumbosacral muscle groups during F-E and LB motions. The psoas muscle in the DS model was subjected to 23.2% greater tensile force than that in the normal model. These findings indicated that L4 anterior slippage and changes in lumbosacral-pelvic alignment affect the biomechanical response of muscles. In summary, the present work demonstrated a certain level of accuracy and validity of our models as well as the differences between the models. Alterations in spondylolisthesis and the accompanying overall imbalance in the spinopelvic complex result in increased loading response levels of the functional spinal units in DS patients, creating a vicious cycle that exacerbates the imbalance in the lumbosacral region. Therefore, clinicians are encouraged to propose specific exercises for the ventral muscles, such as the psoas group, to address spinopelvic imbalance and halt the progression of DS.
Graphical Abstract

Similar content being viewed by others


Explore related subjects
Discover the latest articles and news from researchers in related subjects, suggested using machine learning.Avoid common mistakes on your manuscript.
1 Introduction
Degenerative spondylolisthesis (DS) is a condition with varying degrees of slippage between vertebrae caused by degenerative changes in the intervertebral discs and facet joints. DS is a common condition in elderly individuals and one of the most frequently occurring diseases requiring surgical treatment [1]. Degenerative spine pathology in the United States causes a large economic burden, with direct treatment costs estimated at 80 to 100 billion US dollars per year and additional significant indirect costs of disability and lost work productivity [2, 3]. The US National Health Expenditure is projected to increase 1% faster than the gross domestic product per year for 2017 to 2026 [4]. The prevalence of DS in women is approximately six times greater than that in men, and DS is more common in individuals aged > 45 years [5, 6]. Studies have shown that the overall incidence of DS among middle-aged and elderly people in China is 11.20% [7]. The incidence of slippage involving one vertebral body (Meyerding Grade I) is a common degenerative disc disease, accounting for approximately 90% of DS patients [8]. The most common slippage site is L4-L5, accounting for 73% of DS patients, followed by L5-S1 [9, 10]. As our understanding of the pathophysiology and prognosis of DS has improved, it has become increasingly apparent that this condition encompasses a wide spectrum of biomechanical behaviours.
Despite DS being a representative degenerative disc disease, there are relatively few related biomechanical studies. Ramakrishna et al. [11] developed a normal model of the L1-S1 spine and predicted the tendency of vertebral forwards slippage by reducing the disc height. Yaroub et al. [12] manually decreased the disc height and nucleus area and modelled disc height collapse as a 50% reduction in disc height measured in the mid-sagittal plane by moving the L4 inferiorly while maintaining L4–L5 facet articulation. These studies lack objectivity regarding the disease in clinical patients in their model construction, as DS may also involve other degeneration-related structural defects, such as facet joint hypertrophy, intervertebral disc height loss, and adjacent osteophyte formation [13]. At the same time, some studies have used relatively simplistic approaches for the establishment of biomechanical models involving only the adjacent lumbar vertebrae and not incorporating the complex structure of the pelvis beneath the lumbar spine [14]. Changes in the human lumbar spine are not singular or isolated; there is a complex biomechanical relationship between the lumbar spine and pelvis. The onset of DS is also closely related to the lumbar-pelvic position, thus necessitating a more comprehensive organizational structure in simulation studies. Two clinical studies that compared the spinopelvic parameters with global alignment between DS patients and healthy individuals revealed that the pelvic tilt angle (PT) and pelvic incidence angle (PI) were greater in DS patients than in control individuals (i.e., healthy individuals), and the latter was significantly associated with the degree of vertebral slippage [15, 16]. Additionally, muscle tissues play an important role in governing spinal movement and maintaining stability, but current simulation studies that utilize modelling and solving for muscles are still in their infancy [17]. For example, Zhu et al. [18] investigated the effect of back muscle weakness on DS. However, the back muscles were simplified as having a 200 N compressive load, resulting in the incomplete establishment of muscles.
Currently, related clinical studies are unable to quantitatively assess the biomechanical effects of abnormal structures in DS on biological tissues. Understanding the stress‒strain response of biological tissues can help us make more accurate judgements in disease diagnosis and lead to novel therapeutic targets and comprehensive rehabilitation programs, thereby collectively enhancing therapeutic outcomes for patients. The prime example is the lack of available biomechanical evidence to support and guide the design and optimization of specific exercise prescriptions for patients with DS, since backwards bending is a typical risk factor [19]. Therefore, in this study, we established finite element (FE) models of the lumbar-pelvic complex in both DS patients and normal individuals and conducted a comprehensive simulation study from L1-L5 to the entire pelvis to quantitatively assess the biomechanical response differences between the normal lumbar-pelvic composite model and the DS model. The specific objectives of this study are as follows: (1) to establish finite element models representing the lumbar-pelvic complex in both DS patients and healthy individuals, enabling a direct comparison of biomechanical behaviours, and (2) to quantitatively assess the biomechanical response differences, including load distribution, stress‒strain patterns, and joint kinematics, between the normal and DS models to identify critical biomechanical alterations associated with degenerative spondylolisthesis.
2 Materials and methods
2.1 Development of the FE spinopelvic complex model
2.1.1 Geometry reconstruction
The DS spine model and the normal spine model were established based on female patients and asymptomatic adults, respectively, who were recruited for the experiment. The age, height, weight, and demographic data are detailed in Table 1; we recognize that anatomical variations may impact the results; therefore, it is selected patients and asymptomatic adults of the same ethnicity (Asian), gender (female), and with age, height, and weight differences within 10% for finite element modelling to minimize the impact of anatomical variations, which existing researches have reported that these demographic indicators influenced the mechanical responses of a spine motion segment [20,21,22]. This study was approved by the Medical Ethics Committee of the Fourth Clinical Medical College of Guangzhou University of Chinese Medicine (no. K2022-108–02), and informed consent was obtained from the included subjects. The spinopelvic parameters of the DS patients and asymptomatic adults were measured and evaluated by the same physician using X-ray sagittal views, as shown in Table 2. The PI, PT, sacral slope (SS), and lumbar lordosis (LL) angles were all within the normal range for the healthy adults, while the PI, SS, and LL angles of DS patients were all outside the normal range for healthy adults [23,24,25]. The geometric shapes of the bone structures were extracted from the computed tomography (CT) imaging data of the two groups with an axial interval of 0.60 mm and a sagittal and coronal interval of 0.74 mm. The 3D geometry structure was constructed by using image processing software Mimics (version 19.0), which transformed the dicom format image into a digital model. The model was smoothed, amended, and spherized with Geomagic Studio (version 2015). Then, bone structures were used to generate the solid model in SOLIDWORKS CAD software (version 2021). Soft tissue structures such as intervertebral discs, zygapophyseal cartilage, pubic symphysis, and sacrococcygeal joint cartilage were reconstructed based on anatomical studies [26,27,28,29].
2.1.2 Mesh generation and modelling
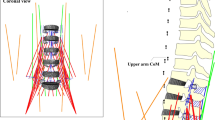
Mesh generation and modelling were performed with HyperMesh software. The generation process in combination with an appropriate mesh resolution allows preservation of morphological features of the biological tissue in the model. The overall FE spinopelvic complex model was developed using Ls-dyna codes (version 11.1.0 × 64, simple precision, SMP), as shown in Fig. 1. The element type selections are listed in Table 3, and numbers of element (nodes) between two models are listed in Table 4.

a View of the normal spine in the 3D reconstructed model. b Spinal function unit of the lumbar spine. c View of the DS spine in the 3D reconstructed model. d L4/5 segment with degenerative change (slippage forward) visible
Functional spinal unit (FSU). Bony structures were modelled by combining shell and solid elements. The cortical bones of each vertebra were modelled with triangular elements to accurately fit the anatomical features, while their thicknesses were based on cadaver data summarized in the literature [30]. The trabecular bone was modelled as tetrahedral elements. The zygapophyseal joint cartilages and bony endplates of the model were generated based on vertebral landmarks and anatomical descriptions [31, 32]. Cappetti et al. [33] reported that geometric parameters significantly affect disc mechanical behaviour, such as sagittal thickness (\({s}_{d}\)), width (\({\overline{w} }_{d}\)), and height (\(H\)) of the disc. In our study, the intervertebral disc modelling parameters are sagittal thickness (\({s}_{d}\)) of 28.79 ± 1.03 mm, width \({\overline{w} }_{d}\) of 43.63 ± 2.24 mm, and height (\(H\)) of 7.96 ± 1.80 mm, which are comparable in geometric size to the spinal segment model parameters reported by Cappetti et al. [33] with differences all within 5%. The facet joints were modelled with triangular elements to accurately fit the anatomy features. The frictionless contacts were defined between the superior and inferior articular cartilages, which were tied to the lateral masses of the vertebrae. The intervertebral discs were modelled as composites of hexahedral bulk element and quadrilateral membrane elements, tied to the vertebral endplates. The intervertebral discs included the components of annulus fibrosus matrix, nucleus pulposus, and annular fibres, which were respectively modelled with hexahedral bulk elements or quadrilateral membrane elements [34]. The intervertebral discs were tied to the adjacent vertebral endplates. The central nucleus pulposus, the anulus fibrosus was four elements in the cranial–caudal direction and two elements in the radial direction. On each layer of the anulus in the radial direction, two layers of membrane elements were superimposed, to represent the nonlinear and orthotropic characteristics of the anulus fibrosus [35, 36]. The cartilaginous endplates were attached to the disc surfaces in the cranial-caudal direction.
Ligaments
In the overall lumbar spine (LS), from L1 to L5, the anterior longitudinal ligament (ALL), posterior longitudinal ligament (PLL), ligamentum flavum (LF), interspinous ligament (ISL), and supraspinal ligament (SSL) were modelled with quadrilateral membrane elements based on anatomical descriptions [37,38,39]. Facet capsular ligaments (FCLs) were modelled with 1D spring elements, and facet cartilage was defined by shell elements. The modelling details of the hip joint capsule were described by Anantha-Krishnan et al. [40]; the joint capsule was modelled as a cylindrical sleeve that originated from an ellipse around the acetabular rim and inserted into an ellipse around the femoral intertrochanteric line. Then, we generated a series of nodes based on anatomical sites [41]. The corresponding nodes in adjacent lines were connected to form 4-node quadrilateral elements along the length of the capsule. The hip joint capsules were subdivided into four longitudinal sectors to approximate the anatomical details.
Muscles
As shown in Fig. 2, the spinopelvic muscles were developed and connected to adjacent bony structures based on a previously published study [36]. Seventy-four of Hill-type 1D elements were used to represent 6 muscle pairs, including the longissimus thoracis pars thoracis, iliacus muscle, quadratus lumborum, musculus iliocostalis, psoas major, and psoas minor, in the spinopelvic complex. The muscle fascicles were redirected at the intermediate vertebrae to better follow the curvature of the spinopelvic structure and upper femurs.

View of the spinopelvic muscles in the FE model (a ventral muscles and b lateral and dorsal muscles)
2.1.3 Material properties
The material properties of the model were based on previous studies, as shown in Table 3. Bone material parameters referenced from classical FE modelling studies, including the whole lumbar spine models by Park et al. [42], Little et al. [43], Rohlmann et al. [44], Goel et al. [45, 46], the ViVA human body model [47, 48], and the GHBMC (Global Human Body Models Consortium) model [49, 50]. Isotropic and kinematic hardening plasticity was used to model the cortical bones, cancellous bones, and bony endplates of the lumbar vertebrae, pelvis, and femurs [36, 51]. Referring to the studies by Zhang et al. [52], the elastic modulus of cortical and trabecular bone was reduced by 33% to represent the degenerative changes in bone mineral density. The nucleus pulposus was modelled with hypoelasticity material [53]. The annulus was built of a multipart material consisting of an annulus fibrosus matrix in a hill foam material [54, 55] and annular fibres with nonlinear orthotropic characteristics [56]. The spinopelvic ligaments were represented by different anatomical thicknesses using orthotropic nonlinear elastic material, as indicated by previously published studies [49,50,51]. Hip joint capsules and symphysis pubis were modelled by linear elastic materials with elastic moduli of 50 MPa and 70 MPa [57,58,59], respectively. The facet cartilage was also modelled using a linear elastic material with an elastic modulus of 10 MPa [60]. Spinopelvic muscles were added to the spinopelvic complex FE model and defined by the improved Hill model. Detailed data such as the origin and insertion points, physiological cross-sectional areas, and muscle segment parameters are available in previous comprehensive dissection studies [36, 61]. Muscle passive properties were determined according to previous studies [48, 62].
2.2 Model validation
The validation matrix of the spinopelvic complex model is illustrated in Table 5. The model was first verified via anatomical measurements. Then, it was validated step by step from the isolated tissues to the segments. For all the conducted simulations, gravity loading (a volume load of 9.81 m/s2) was included. The simulation details are described as follows.
2.2.1 Compression test
First, as described by Wagnac et al. [63, 64], a uniform axial displacement rate of 0.1 m/s (low dynamic loading) and 1.0 m/s (high dynamic loading) for the superior nodes of the vertebral body was used to evaluate the stiffness of the vertebral body. The simulated force–displacement curve was compared with that of the experimental corridor.
2.2.2 Tension tests
Tension tests were performed on the ALL, PLL, LF, ISL, SSL, and FCL. The respective force‒displacement curves were compared with the experimental data from Wagnac et al. [63, 64].
2.2.3 6-DOF moment of functional spinal units
Next, the motion characteristics of the model were verified in three rotation directions as described in previous studies [44, 65]. For the entire lumbar spine and each FSU, moments were applied to the superior portion of the L1 at 3.75 Nm and 7.50 Nm for flexion–extension (F-E), lateral bending (LB), and axial rotation (AR), as described in previous studies [44, 65]. The respective moment–rotation simulation curves were compared with the experimental ranges.
2.2.4 Shear test for the DS model
Lateral shear tests were performed on the cranial vertebra relative to the caudal vertebra of L4, since L4/5 is the slippage segment in the DS model. The pure LB moments were applied at 5 Nm in accordance with the load increments in the study by Melnyk et al. [66]. In addition, the L4/5 DS model was subjected to anterior shear and posterior shear to the cranial vertebra. The moment–rotation simulation curves and force–translation curves were compared with the experimental data [66].
All simulations were run with single-precision LS-DYNA codes (version 11.1.0 × 64, simple precision, SMP). The bilateral femurs were constrained in all directions. General contact was enforced for the entire model. The motion characteristics of the segments and the intervertebral discs as well as the vertebral loads were analysed. A global coordinate system with X to the left, Y backwards, and Z upwards was utilized. Finally, to explore the biomechanical differences in DS involvement under different loading modes, the responses of the spinopelvic kinematics and important adjacent tissues or segments were compared between the normal spinopelvic FE model and DS spinopelvic model.
3 Results
3.1 Validation of the spinopelvic FE model
3.1.1 Compression test
The vertebrae were subjected to compressive tests, simulating force‒displacement curves that ranged from high-dynamic (HD) to low-dynamic (LD) conditions. The results of this comprehensive evaluation are illustrated in Fig. 3a, b. Under HD conditions, a substantial reaction force of 5605.3 N was recorded at a displacement of 3.7 mm. The simulated force‒displacement curves and the experimental values were similar, exhibiting a monotonic increasing trend, with the peak values being nearly consistent. Under LD conditions, a lower reaction force of 1902.0 N was observed at a displacement of 6.5 mm. The simulated force‒displacement curve for LD was scattered within the experimental range.

3.1.2 Isolated tissues
In spinopelvic ligament tension tests, most of the force–displacement curves for the normal model were within the experimental corridor concerning both curve shapes and peak values, as shown in Fig. 4. Most simulated force‒displacement curves could be described as a distinctive J-shaped curvature up to the peak load and exhibited regions of toe, linear, and traumatic motion in the process of tension. The PLL simulation curve exhibited an asymmetric sigmoidal shape up to the peak load. The validated results delineated the range of the ultimate load capacity of the spinopelvic ligaments, which spanned from approximately 59.8 to 411.5 N. This wide range reflects the significant variability in the mechanical strength of different ligaments within the spinopelvic framework, highlighting the complex interplay of forces that these structures can withstand in vivo.

3.1.3 6-DOF moment of functional spinal units
For entire spinopelvic FSU rotation analysis, this study employed a comprehensive 6-DOF rotational analysis to elucidate the biomechanical responses to pure moments. The corresponding full moment–rotation responses, encapsulated in the normal spinopelvic model, are meticulously documented in Figs. 5 and 6, including the F-E, LB, and AR loading conditions. The pure moments were set as 3.75 Nm and 7.5 Nm for assessing the ROM within the spinal segments, providing a detailed comparative analysis against established experimental corridors. In the F-E, LB, and AR loading conditions with pure moments of 3.75 Nm and 7.5 Nm, most of the ROMs were within the experimental corridors for both curve shapes and peak values. This congruence underscores the reliability and accuracy of the simulation model in replicating the physiological and biomechanical properties of spinopelvic FSUs under dynamic loading conditions. Additionally, the ROMs of the separated FSUs in the entire spinopelvic FE model were all within one standard deviation of the experimental data [65] for loading with pure moments of 7.5 Nm, as shown in Fig. 7.

Moment–displacement curve validation of the normal spinopelvic model for loading with pure moments of 3.75 Nm in a flexion–extension, b lateral bending, and c axial rotation compared with Rohlmann et al. [44]

Moment–displacement curve validation of the normal spinopelvic model for loading with pure moments of 7.5 Nm in a flexion–extension, b lateral bending, and c axial rotation compared with Rohlmann et al. [44]

7.5 Nm moment histogram validation of each segment (L1-S1) in the normal spinopelvic model under a flexion–extension, b lateral bending, and c axial rotation compared with Cook et al. [65]
3.1.4 Shear test for the DS model
In the intricate field of biomechanical engineering, particularly in the analysis of the DS model, the shear test has emerged as a critical methodological approach to assess mechanical behaviour under varying load conditions. This study compared moment–rotation simulation curves and force–displacement curves against experimental data [66], thereby providing a robust model for evaluating the predictive accuracy and reliability of the DS spine under shear stress conditions. The comparative analyses are graphically presented in Fig. 8. The moment–rotation simulation curve (Fig. 8a) exhibited an asymmetric S-shape, and the majority of the curve fell within the experimental corridor. The anterior–posterior translation had a relatively linear relationship with the shear force across the shear loading conditions, as shown in Fig. 8b. Although the peak value of the anterior shear curve in the DS model was slightly lower than the experimental peak value, the tendency was consistent with that of the experimental curve. The simulation results and experimental findings aligned closely, particularly in the context of posterior shear loading.

3.2 Comparison of the normal spine model and DS spine model
The peak stress of the lumbar isthmic-cortical bones, intervertebral discs, and facet joints; the peak strain of ligaments; the peak force of muscles; and the percentage difference in the ROM during F-E, LB, and AR motions were analysed and compared between the normal spine model and the DS spine model.
3.2.1 Lumbosacral intervertebral disc stress
The peak stress of the intervertebral discs under F-E, LB, and AR conditions was greater than that in the normal model. As shown in Fig. 9a, in the comparison of the peak stress on the L4/5 intervertebral disc (Fig. 9a), under the influence of L4/5 segment slippage, the stress in the DS spine model was greater than that in the normal model; under F-E, LB, and AR conditions, the stress was 1.6, 1.1, and 6.6 times greater than that in the normal model, respectively. In the normal spine model, the least stress on the intervertebral disc occurred under the AR condition, whereas in the DS spine model, the highest stress was observed under the AR condition. Following disc slippage, there is a decrease in the segment’s ability to resist AR motion, a pattern that also becomes apparent during F-E motion. A comparison of the peak stress in the L5/S1 intervertebral disc between the DS and normal spine models revealed minor differences, as shown in Fig. 9b. However, under LB and AR conditions, the peak stress of the normal model at the L5/S1 disc was still 16.18% and 14.84% lower, respectively, than that of the DS spine model.

Comparison of peak stress in a L4/5 intervertebral disc and b L5/S1 intervertebral disc between normal spine model and DS spine model
3.2.2 L4 cortical bone von Mises stress and typical stress distribution nephograms
As illustrated in Fig. 10, we compared the peak stress of the L4 cortical bone between the two models under F-E, LB, and AR conditions. In terms of the distribution of peak stress in the L4 cortical bone under different conditions, the values for the DS spine model were consistently greater than those for the normal model; the peak stress was 1.2, 2.1, and 1.7 times greater under F-E, LB, and AR conditions, respectively. The peak stress presented by the L4 cortical bone in the DS spine model was the greatest during axial rotation. According to the typical stress distribution nephograms of flexion motion (Fig. 11), the overall stress region of the DS spine model was greater than that of the normal spine model. The former showed more high-stress areas than did the latter, especially in anatomical structures prone to stress concentration, such as the facet joint isthmus, where the DS spine model exhibited greater peak stress than did the normal spine model. Additionally, forwards slippage of the L4/5 pathological segment caused a shift in the high-stress distribution nephogram of the vertebrae towards the vertebral pedicle and anterior edge of the lamina.

Comparison of peak stress in L4 cortical bone between DS spine model and normal spine model

Comparison of typical von Mises stress (GPa) distribution nephograms (flexion motion) between two models. a Top view of L4 in normal spine model. b Top view of L4 in DS spine model. c Rear view of L4 in normal spine model. d Rear view of L4 in DS spine model
3.2.3 Percentage differences in L4/5 and L5/S1 ROMs
Comparison of the percentage differences in mobility levels of the L4/5 and L5/S1 segments between the normal spine model and the DS spine model clearly illustrates the disparities in segment stability between the models. As shown in Fig. 12, both the L4/5 and L5/S1 segments were significantly greater in the DS spine model than in the normal spine model, indicating that slippage pathology affects segment stability. The greatest impacts primarily occurred during AR and LB motions, followed by the F-E motion. This finding suggested that after anterior vertebral slippage, the pathological segment mainly exhibited reduced abilities to resist AR and LB motions. The comparison between the two models in terms of the percentage difference in the L5/S1 ROM reflected a similar trend, although segments without DS did not show compromised stability during F-E motion.

Comparison of percentage difference of L4/5 and L5/S1 ROM between the normal spine model and DS spine model
3.2.4 Peak stress of the L4/5 facet joint and peak strain of the spinal ligaments
Given the notable differences in biomechanical responses to LB and AR motions between the normal spine model and DS spine model and considering the vital anatomical function of the facet joints in resisting LB and AR motions, we compared the stress differences in the L4/5 facet joints of the two models. As shown in Fig. 13, a substantial disparity in facet joint stress was observed between the two models, with the DS spine model consistently showing greater stress than the normal model across the three conditions, specifically, 1.3, 6.6, and 1.9 times greater for the F-E, LB, and AR loading conditions, respectively.

Comparison of L4/5 facet joint peak stress between normal spine model and DS spine model
Compared to the loading conditions of F-E, LB, and AR (Fig. 14), the peak strain values of the ligaments in the DS spine model were greater than those in the normal spine model. The peak strain of the PLL in the DS spine model was the highest among all the tested spinal ligaments and was notably greater than that in the normal spine model. The PLL peak strain of the normal model was only 1/10 that of the DS model, indicating that the PLL is the most susceptible ligament that is significantly affected after anterior vertebral slippage. In addition, a pronounced disparity was also evident in the peak strain of the ISL between the two models. A notable difference in the peak strain of the ISL was observed between the two models, particularly for the F-E and AR motions.

Comparison of L4/5 ligaments peak strain between the normal spine model and DS spine model. (a) Under FE loading condition. (b) Under LB loading condition. (c) Under AR loading condition
3.2.5 Muscle tensile force in the lumbosacral region
As shown in Fig. 15, a comparison of forces under six conditions revealed that the trends in muscle tensile forces were generally similar between the two models. However, most muscle tensile forces in the lumbosacral region of the DS spine model were greater than those in the normal model, except the iliacus muscle. The psoas muscle and iliocostalis muscle exhibited the greatest tensile forces in the two spinopelvic complex models. During spine extension, the psoas muscle in the DS spine model was subjected to 23.2% greater tensile force than that in the normal spine model. Under LB loading conditions, the iliocostalis muscle in the DS spine model also exhibited a 42.2% greater tensile force than that of the normal spine model. Compared with those of the normal spine model, the tensile force of the quadratus muscle of the DS model increased by 34.7%. Overall, the DS model exhibited greater muscle tensile forces in the lumbosacral muscle groups during F-E and LB motions than did the normal model, indicating that L4 anterior slippage and changes in lumbosacral-pelvic alignment significantly affected the biomechanical response of the muscles. The comparative muscle nephograms in Fig. 16 illustrate the tensile forces on the psoas during extension in both models, revealing that the muscle tension in the DS spine model exceeded that in the normal model, with a force concentration on the DS pathological segment and its proximal segments.

Comparison of muscle (iliacus, quadratus, longissimus thoracis, psoas, and iliocostalis) tensile force of lumbosacral region between normal spine model and DS spine model

Comparative muscle nephograms of the muscle tensile forces on the psoas during extension between a normal spine model and b DS spine model
4 Discussion
Based on the development and validation of a new spinopelvic complex FE model with muscle modelling, the present study simulated an in vivo response of the human spinopelvic system and analysed the effects of DS with abnormal spinopelvic parameters on lumbosacral kinematics. Due to the pathological changes involved in vertebral slippage in the DS model and the corresponding changes in spinopelvic positional parameters, alterations were observed in muscular and skeletal structures, tissue strain, stress levels, segmental ROM, and load concentration locations. Compared to the results of cadaveric experiments, the validated analysis demonstrated the biofidelity of our normal spine model, as shown in Figs. 3, 4, 5, 6, and 7. Moreover, limited studies have recorded scattered data, which are also well correlated with the present DS model. As shown in Fig. 8, the DS model showed segmental moment–rotation curves and force–displacement curves mostly within the experimental corridor and consistent with the curve trend.
While several studies have addressed the biomechanical effects of DS, previous computational models have been limited to isolated lumbar spine studies and simplified musculature. Yaroub et al. [12] reconstructed the FSU of the fourth and fifth lumbar vertebrae with spondylolysis and reported that AR motion was associated with the most significant increase in the ROM in an isthmic spondylolisthesis model, which was consistent with our finding that the DS spine model displayed hypermobility in terms of flexion and rotation. Liu et al. [67] also developed a L3-S1 FE model and demonstrated that intradiscal pressure was increased in the DS spine model, indicating a greater possibility of disc degeneration. However, they did not use a suitable method of validation for the spondylolisthesis model, as it was developed by extending the isthmus of the normal lumbar spine, which may not accurately reflect the morphological characteristics of lower-grader DS. Only one study evaluated the effects of back muscles (simplified as a 200 N compressive load) on DS, which could impact the robustness of the conclusions [18]. A more detailed model including additional muscles would be beneficial for determining the biomechanical effects of abnormal DS structures on biological tissues. In this study, a DS spine model was reconstructed from a real DS patient whose age, height, and weight were within 10% of those in the normal spine model. However, significant differences in the spinal-pelvic parameters existed between the two models, with the PI, SS, LL, and PT parameters in the DS spine being greater than those in the normal spine, while the first three parameters even exceeded the normal ranges. Changes in the spinopelvic structure of DS cause alterations in adjacent skeletal muscles, combined with progressive degenerative changes in the pathological segments. Additionally, changes in the line of force applied to the spinopelvic structure, which causes changes in the sagittal plane alignment of the spine, have been implicated in the development and progression of DS. Barrey et al. [68] proposed that an increase in the SS and PI angles from the normal reference values was predictive of DS. In agreement with these findings, Curylo et al. [69] reported a significantly greater PI among fifty-three patients with DS than among a control group. Labelle et al. [70] also reported greater LL values among patients with DS, with an increase in this parameter being positively correlated with the grade of spondylolisthesis. These studies confirm a relationship between DS and spinopelvic parameters of sagittal plane alignment, with an increase in the PI and LL being specifically associated with DS. Therefore, when numerically modelling and analysing the DS model, it is crucial to consider the positional parameters of the lumbar pelvis. Global sagittal balance has unique biomechanical effects on the biological tissues of pathological segments and their adjacent segments in the DS model.
Regarding the intervertebral discs, the two models showed substantial differences concerning both peak stress values, as shown in Fig. 9. Under the influence of L4 forwards slippage, the peak stress of the L4/5 intervertebral disc in the DS spine model under the AR condition was 6.6 times greater than that in the normal spine model. Following disc slippage, the ability of the segment to resist AR motion decreases, and this tendency also becomes apparent with slippage at the L5/S1 segment. Following degenerative changes in the intervertebral disc, the height of the disc space decreases, the structure of the endplate deforms, and the ability of the disc to absorb shocks and distribute loads evenly across the endplate decreases, ultimately reducing the resistance of the disc to AR motion. The primary biomechanical function of the intervertebral disc is to resist compressive forces, and its overall structure is not conducive to withstanding other types of loads; it is especially poor at tolerating torsional stress [71]. Additionally, the increased peak stress in the intervertebral discs of spondylolisthesis patients and the adjacent segments also influences posterior facet joints, which are crucial anatomical structures in the functional spinal unit opposing LB and AR motions. As DS often accompanies an increase in lumbar pelvic parameters, the increased shear forces in the segment also increase the stress on facet joints and intervertebral discs. Labelle et al. [72] reported that a linear association existed between the PI and spinal spondylolisthesis. Lv et al. [73] reported that patients with increased PI values are at a greater risk of DS, and an increase in PI leads to elevated mechanical stress on lumbar facet joints. Our results also indicated that the facet joint stress in the L4/L5 pathological segments of the DS spine model was notably greater than that in the normal spine model.
Increased stress on the facet joints and intervertebral discs suggested a greater ROM during LB and AR motions in the DS spine model, as shown in Fig. 12. The reported data indicated that segmental motion was greater in patients with moderate facet joint and disc degeneration than in normal subjects [74]. Increased mechanical stress on the three-joint complex in the functional spinal unit leading to segmental instability is an important cause of low back pain, potentially accelerating tissue degeneration, including hypertrophy of the facet joints and further reduction in disc space height, resulting in the redistribution of stress as the biological tissues attempt to achieve segmental adaptive stabilization [75]. Our findings also suggest that the ROM in the F-E motion of segments following vertebral forwards slippage is only slightly greater than that in the normal spine model. Changes following DS also cause stress alterations, as illustrated by the typical stress distribution nephograms in Fig. 11. Under flexion motion, the DS spine model showed more high-stress areas than did the normal spine model, especially in anatomical structures prone to stress concentration, such as the facet joint isthmus, where the DS spine model exhibited greater peak stresses than did the normal spine model. Additionally, forwards slippage of the vertebra resulted in increased strain on the posterior spinal ligaments, notably the PLL and ISL. Overall, the trend in changes in peak ligament strain indicated that the DS spine model exhibited obviously greater strain than the normal spine model.
The natural history of DS is generally favourable. Only 10–15% of patients seeking treatment will eventually undergo surgery [76]. Therefore, for patients with DS, conservative treatment remains the primary therapeutic approach in current clinical practice. Overuse of the stabilization muscles may cause or aggravate forwards slipping in DS patients. However, little biomechanical evidence is available to explain the mechanism underlying exercise therapy [18]. Merely strengthening the back muscles appears to be insufficient because DS is often accompanied by an anterior pelvic tilt and an increased lordotic angle of the lumbar spine, resulting in the shortening and tightening of anterior muscles such as the psoas. As these weakened muscles stay in that position, they need to work extra hard to stabilize the pelvis and core, causing them to tighten. This study demonstrated that changes in the pelvic tilt affect the length of the muscles around the spine and hip joint. These muscles often become inactive due to the prolonged sitting that occurs in modern life and work. In this study, we found that most muscle tensile forces in the lumbosacral region of the DS spine model were greater than those in the normal model. During spine extension, the psoas in the DS spine model was subjected to 23.2% greater tensile force than that in the normal spine model. Compared with that of the normal spine model, the tensile force of the quadratus muscle of the DS model increased by 34.7%. This result indicates that during the muscle strengthening process in DS patients, it is necessary to strengthen both the ventral and dorsal musculature of the spine-pelvis, whereas most current clinical practices focus primarily on the dorsal muscles [77], inadvertently exacerbating the imbalance in the antagonist muscle groups. In fact, weakness in the abdominal muscles is observed in most patients with low back pain. The anatomical position of the psoas major is very close to the axis of motion of the lumbar spine and hip joint, thereby aiding in maintaining the stability and coaxial alignment of the lumbar spine and hip joints [26, 78]. A weakened psoas in the hip joint can cause problems with balance and posture control during activities. Kim et al. [79] reported that a change in the pelvic tilt influences the alignment of the spine and causes great stress on the lumbar vertebrae, which is consistent with our simulated results. Therefore, this study provides quantitative data to emphasize the importance of exercising the ventral muscle groups in DS patients, aimed at correcting the pelvic position to improve posture.
The limitations of this study should be noted. The absence of active muscular contraction prevented direct evaluation of lumbar spine motion [80, 81]. However, defining active muscle forces in DS patients is particularly challenging due to the complexity and variability of muscle activation patterns in this condition. Neglecting this effect is a simplification used in the present work, which should be considered in future improvements of our model. Additionally, changes in size and shape of bones and tissue may affect magnitude and even quality of the results reported. In this study, by controlling these critical influencing variables, we aim to minimize differences in vertebral size, shape, and other morphological characteristics. The modelling of the DS spine reflects clinical authenticity derived from actual DS patient, and the model has been validated through cadaveric experiments. This methodology obtains model’s biofidelity to a certain degree. In the future, we will utilize spatial interpolation methods, such as Kriging, to establish the FE models. Finally, the vertebrae [82, 83], intervertebral disc, and other tissue materials in the FE model of the lumbar-pelvic complex do not represent the state-of-the-art constitutive equations, which may affect the quantitative data of the simulation results. A notable example includes the annulus fibrosus, which are recently based on biphasic or biphasic-swelling theories [84,85,86,87,88]. These models offer the advantage of simulating fluid–solid interactions and osmotic pressure. The annulus fibrosus modelling of this study is the lack of comprehensive integration among fluid–solid interaction (permeability), the impact of biochemical components (hydration), regional variations in structural arrangement, and mechanical properties of both collagen and elastic fibres (fibre reinforcement). In this study, degenerative spondylolisthesis mainly involves structural disc and facet joints degeneration, while material degeneration, which is also critically important, was not addressed. However, this study is able to show the general trends of load transfers between the DS spine and the healthy spine. More reliable material properties and more accurate geometries by utilizing in vivo experiments, such as Amirouche et al. [89], focusing on DS subjects are needed in order to increase the biomechanical predictive capability and clinical utility of any future the FE models.
5 Conclusion
The present study established, validated, and compared normal spine and DS models based on detailed FE spinopelvic complex models with muscle modelling. The obvious simulation differences indicated greater peak stress in the intervertebral discs of the pathological segment and adjacent segments in DS patients with than in those of the normal spine, as well as overall greater ligament strain and facet joint stress. This is particularly evident during axial rotation of the spondylolisthesis spine. Biomechanical differences originate not only from alterations in the spondylolisthesis segment but also from an overall imbalance in the spinopelvic complex. Forwards vertebra slippage and greater spinopelvic parameters also result in more high-stress areas, such as the isthmus region, and stress-concentrated locations are evidently transferred forwards. Finally, this study provided a quantitative biomechanical comparison to emphasize the importance of exercises targeting the psoas and other ventral muscles for DS patients to improve the pathological state of anterior pelvic tilt and prevent the progression of DS.
References
Harrop JS, Hilibrand A, Mihalovich KE, Dettori JR, Chapman J (2014) Cost-effectiveness of surgical treatment for degenerative spondylolisthesis and spinal stenosis. Spine 39(22 Suppl 1):S75-85. https://doi.org/10.1097/brs.0000000000000545
Martin BI, Deyo RA, Mirza SK, Turner JA, Comstock BA, Hollingworth W et al (2008) Expenditures and health status among adults with back and neck problems. JAMA 299(6):656–664. https://doi.org/10.1001/jama.299.6.656
Dagenais S, Caro J, Haldeman S (2008) A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J Off J North Am Spine Soc 8(1):8–20. https://doi.org/10.1016/j.spinee.2007.10.005
Jones KE, Polly DW Jr (2019) Cost-effectiveness for surgical treatment of degenerative spondylolisthesis. Neurosurg Clin N Am 30(3):365–372. https://doi.org/10.1016/j.nec.2019.02.010
Koreckij TD, Fischgrund JS (2015) Degenerative spondylolisthesis. 28(7):236-41. https://doi.org/10.1097/bsd.0000000000000298
Derman PB, Albert TJ (2017) Interbody fusion techniques in the surgical management of degenerative lumbar spondylolisthesis. Curr Rev Musculoskelet Med 10(4):530–538. https://doi.org/10.1007/s12178-017-9443-2
Liu Z, Qin X, Sun K, Yin H, Chen X, Yang B et al (2022) Manipulation for degenerative lumbar spondylolisthesis: a systematic review of randomized controlled trials. J Tradit Chin Med Sci 9(2):121–127. https://doi.org/10.1016/j.jtcms.2022.02.001
Aoki Y, Takahashi H, Nakajima A, Kubota G, Watanabe A, Nakajima T et al (2020) Prevalence of lumbar spondylolysis and spondylolisthesis in patients with degenerative spinal disease. Sci Rep 10(1):6739. https://doi.org/10.1038/s41598-020-63784-0
Akkawi I, Zmerly H (2022) Degenerative spondylolisthesis: a narrative review. Acta bio-medica Atenei Parmensis 92(6):e2021313. https://doi.org/10.23750/abm.v92i6.10526
Koslosky E, Gendelberg D (2020) Classification in brief: the Meyerding classification system of spondylolisthesis. Clin Orthop Relat Res 478(5):1125–1130. https://doi.org/10.1097/corr.0000000000001153
Ramakrishna VAS, Chamoli U, Viglione LL, Tsafnat N, Diwan AD (2018) Mild (not severe) disc degeneration is implicated in the progression of bilateral L5 spondylolysis to spondylolisthesis. BMC Musculoskelet Disord 19(1):98. https://doi.org/10.1186/s12891-018-2011-0
Yaroub S, Hamandi SJ, Mohson K (2022) Kinematic analysis of L4–L5 spinal segment with spondylolysis and different types of grade 1 spondylolisthesis: a nonlinear finite element study. Acta Bioeng Biomech 24(2):177–186
Bashkuev M, Reitmaier S, Schmidt H (2020) Relationship between intervertebral disc and facet joint degeneration: a probabilistic finite element model study. J Biomech 102:109518. https://doi.org/10.1016/j.jbiomech.2019.109518
Ding H, Liao L, Yan P, Zhao X, Li M (2021) Three-dimensional finite element analysis of l4–5 degenerative lumbar disc traction under different pushing heights. J Healthc Eng 2021:1322397. https://doi.org/10.1155/2021/1322397
Oh SK, Chung SS, Lee CS (2009) Correlation of pelvic parameters with isthmic spondylolisthesis. Asian Spine J 3(1):21–26. https://doi.org/10.4184/asj.2009.3.1.21
Gadkari A, Ghodke A, Jha A (2022) Correlation of pelvic incidence and pelvic parameters in lumbar spondylolisthesis. Surg Neurol Int 13:405. https://doi.org/10.25259/sni_545_2022
Zhu R, Niu WX, Wang ZP, Pei XL, He B, Zeng ZL et al (2018) The effect of muscle direction on the predictions of finite element model of human lumbar spine. Biomed Res Int 2018:4517471. https://doi.org/10.1155/2018/4517471
Zhu R, Niu WX, Zeng ZL, Tong JH, Zhen ZW, Zhou S et al (2017) The effects of muscle weakness on degenerative spondylolisthesis: a finite element study. Clin Biomech (Bristol Avon) 41:34–38. https://doi.org/10.1016/j.clinbiomech.2016.11.007
Vanti C, Ferrari S, Guccione AA, Pillastrini P (2021) Lumbar spondylolisthesis: state of the art on assessment and conservative treatment. Arch Physiother 11(1):19. https://doi.org/10.1186/s40945-021-00113-2
Sawa AGU, Lehrman JN, Crawford NR, Kelly BP (2020) Variations among human lumbar spine segments and their relationships to in vitro biomechanics: a retrospective analysis of 281 motion segments from 85 cadaveric spines. Int J Spine Surg 14(2):140–50. https://doi.org/10.14444/7021
Bruno AG, Broe KE, Zhang X, Samelson EJ, Meng CA, Manoharan R et al (2014) Vertebral size, bone density, and strength in men and women matched for age and areal spine BMD. J Bone Mineral Res Off J Am Soc Bone Mineral Res 29(3):562–569. https://doi.org/10.1002/jbmr.2067
Miller CA, Hwang SJ, Cotter MM, Vorperian HK (2021) Developmental morphology of the cervical vertebrae and the emergence of sexual dimorphism in size and shape: a computed tomography study. Anat Rec (Hoboken, NJ : 2007) 304(8):1692–708. https://doi.org/10.1002/ar.24559
Zhu Z, Xu L, Zhu F, Jiang L, Wang Z, Liu Z et al (2014) Sagittal alignment of spine and pelvis in asymptomatic adults: norms in Chinese populations. Spine 39(1):E1-6. https://doi.org/10.1097/brs.0000000000000022
Zhou S, Sun Z, Li W, Zou D, Li W (2022) The pelvic incidence stratified sagittal spinopelvic alignment in asymptomatic Chinese population with different age groups. Glob Spine J 12(8):1821–1826. https://doi.org/10.1177/2192568221989647
Lin RM, Jou IM, Yu CY (1992) Lumbar lordosis: normal adults. J Formos Med Assoc = Taiwan yi zhi 91(3):329–33
Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH (2012) The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat 221(6):537–567. https://doi.org/10.1111/j.1469-7580.2012.01564.x
Woon JT, Stringer MD (2012) Clinical anatomy of the coccyx: a systematic review. Clinical anatomy (New York, NY) 25(2):158–167. https://doi.org/10.1002/ca.21216
Mengoni M (2021) Biomechanical modelling of the facet joints: a review of methods and validation processes in finite element analysis. Biomech Model Mechanobiol 20(2):389–401. https://doi.org/10.1007/s10237-020-01403-7
Yao J, Dong B, Sun J, Liu JT, Liu F, Li XW et al (2020) Accuracy and reliability of computer-aided anatomical measurements for vertebral body and disc based on computed tomography scans. Orthop Surg 12(4):1182–1189. https://doi.org/10.1111/os.12729
Palepu V, Rayaprolu SD, Nagaraja S (2019) Differences in trabecular bone, cortical shell, and endplate microstructure across the lumbar spine. Int J Spine Surg 13(4):361–70. https://doi.org/10.14444/6049
Wang Y, Battié MC, Videman T (2012) A morphological study of lumbar vertebral endplates: radiographic, visual and digital measurements. Eur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc 21(11):2316–2323. https://doi.org/10.1007/s00586-012-2415-8
Inoue N, Orías AAE, Segami K (2020) Biomechanics of the lumbar facet joint. Spine Surg Relat Res 4(1):1–7. https://doi.org/10.22603/ssrr.2019-0017
Cappetti N, Naddeo A, Naddeo F, Solitro GF (2010) Influence of the disk geometry on different FEM models of the spine. 9th international symposium on Computer Methods in Biomechanics and Biomedical Engineering, Valencia (SPAIN). 24–7
Panzer MB, Cronin DS (2009) C4–C5 segment finite element model development, validation, and load-sharing investigation. J Biomech 42(4):480–490. https://doi.org/10.1016/j.jbiomech.2008.11.036
Liang Z, Mo F, Zheng Z, Li Y, Tian Y, Jiang X et al (2022) Quantitative cervical spine injury responses in whiplash loading with a numerical method of natural neural reflex consideration. Comput Methods Programs Biomed 219:106761. https://doi.org/10.1016/j.cmpb.2022.106761
Xu G, Liang Z, Tian T, Meng Q, Bertin KM, Mo F (2023) Development of a finite element full spine model with active muscles for quantitatively analyzing sarcopenia effects on lumbar load. Comput Methods Programs Biomed 240:107709. https://doi.org/10.1016/j.cmpb.2023.107709
Wiczenbach T, Pachocki L, Daszkiewicz K, Łuczkiewicz P, Witkowski W (2023) Development and validation of lumbar spine finite element model. PeerJ 11:e15805. https://doi.org/10.7717/peerj.15805
Scapinelli R, Stecco C, Pozzuoli A, Porzionato A, Macchi V, De Caro R (2006) The lumbar interspinous ligaments in humans: anatomical study and review of the literature. Cells Tissues Organs 183(1):1–11. https://doi.org/10.1159/000094901
Lawrence S, Llewellyn S, Hunt H, Cowin G, Sturgess DJ, Reutens D (2021) Anatomy of the lumbar interspinous ligament: findings relevant to epidural insertion using loss of resistance. Reg Anesth Pain Med 46(12):1085–1090. https://doi.org/10.1136/rapm-2021-103014
Anantha-Krishnan A, Myers CA, Fitzpatrick CK, Clary CW (2023) Instantaneous generation of subject-specific finite element models of the hip capsule. Bioengineering (Basel, Switzerland) 11(1):37. https://doi.org/10.3390/bioengineering11010037
Anantha Krishnan A, Myers CA, Scinto M, Marshall BN, Clary CW (2023) Specimen-specific finite element representations of implanted hip capsules. Comput Methods Biomech Biomed Eng 27(6):1–14. https://doi.org/10.1080/10255842.2023.2200878
Park WM, Kim K, Kim YH (2013) Effects of degenerated intervertebral discs on intersegmental rotations, intradiscal pressures, and facet joint forces of the whole lumbar spine. Comput Biol Med 43(9):1234–1240. https://doi.org/10.1016/j.compbiomed.2013.06.011
Little JP, de Visser H, Pearcy MJ, Adam CJ (2008) Are coupled rotations in the lumbar spine largely due to the osseo-ligamentous anatomy?–a modeling study. Comput Methods Biomech Biomed Eng 11(1):95–103. https://doi.org/10.1080/10255840701552143
Rohlmann A, Neller S, Claes L, Bergmann G, Wilke HJ (2001) Influence of a follower load on intradiscal pressure and intersegmental rotation of the lumbar spine. Spine 26(24):E557–E561. https://doi.org/10.1097/00007632-200112150-00014
Goel VK, Mehta A, Jangra J, Faizan A, Kiapour A, Hoy RW et al (2007) Anatomic facet replacement system (AFRS) restoration of lumbar segment mechanics to intact: a finite element study and in vitro cadaver investigation. SAS J 1(1):46–54. https://doi.org/10.1016/sasj-2006-0010-rr
Dreischarf M, Zander T, Shirazi-Adl A, Puttlitz CM, Adam CJ, Chen CS et al (2014) Comparison of eight published static finite element models of the intact lumbar spine: predictive power of models improves when combined together. J Biomech 47(8):1757–1766. https://doi.org/10.1016/j.jbiomech.2014.04.002
Östh J, Brolin K, Svensson MY, Linder A (2016) A female ligamentous cervical spine finite element model validated for physiological loads. J Biomech Eng 138(6):061005. https://doi.org/10.1115/1.4032966
Östh J, Mendoza-Vazquez M, Sato F, Svensson MY, Linder A, Brolin K (2017) A female head-neck model for rear impact simulations. J Biomech 51:49–56. https://doi.org/10.1016/j.jbiomech.2016.11.066
Davis ML, Koya B, Schap JM, Gayzik FS (2016) Development and full body validation of a 5th percentile female finite element model. Stapp Car Crash J 60:509–544. https://doi.org/10.4271/2016-22-0015
Schwartz D, Guleyupoglu B, Koya B, Stitzel JD, Gayzik FS (2015) Development of a computationally efficient full human body finite element model. Traffic Inj Prev 16(Suppl 1):S49-56. https://doi.org/10.1080/15389588.2015.1021418
Liang Z, Xu G, Liu T, Zhong Y, Mo F, Li Z (2023) Quantitatively biomechanical response analysis of posterior musculature reconstruction in cervical single-door laminoplasty. Comput Methods Programs Biomed 233:107479. https://doi.org/10.1016/j.cmpb.2023.107479
Zhang XY, Han Y (2023) Comparison of the biomechanical effects of lumbar disc degeneration on normal patients and osteoporotic patients: a finite element analysis. Med Eng Phys 112:103952. https://doi.org/10.1016/j.medengphy.2023.103952
Lin M, Paul R, Dhar UK, Doulgeris J, O’Connor TE, Tsai CT et al (2023) A review of finite element modeling for anterior cervical discectomy and fusion. Asian Spine J 17(5):949–963. https://doi.org/10.31616/asj.2022.0295
Campana S, Charpail E, de Guise JA, Rillardon L, Skalli W, Mitton D (2011) Relationships between viscoelastic properties of lumbar intervertebral disc and degeneration grade assessed by MRI. J Mech Behav Biomed Mater 4(4):593–599. https://doi.org/10.1016/j.jmbbm.2011.01.007
Yan Y, Huang J, Li F, Hu L (2018) Investigation of the effect of neck muscle active force on whiplash injury of the cervical spine. Appl Bionics Biomech 2018:4542750. https://doi.org/10.1155/2018/4542750
Shen T-WD (2020) Investigation of whiplash associated disorders using finite element neck models with active musculature in frontal, rear and lateral impact. UWSpace
Hewitt J, Guilak F, Glisson R, Vail TP (2001) Regional material properties of the human hip joint capsule ligaments. J Orthop Res Off Publ Orthop Res Soc 19(3):359–364. https://doi.org/10.1016/s0736-0266(00)00035-8
Duquesne K, Pattyn C, Vanderstraeten B, Audenaert EA (2022) Handle with care: the anterior hip capsule plays a key role in daily hip performance. Orthop J Sports Med 10(3):23259671221078256. https://doi.org/10.1177/23259671221078254
Watson PJ, Fagan MJ, Dobson CA (2015) Sensitivity to model geometry in finite element analyses of reconstructed skeletal structures: experience with a juvenile pelvis. Proc Inst Mech Eng Part H J Eng Med 229(1):9–19. https://doi.org/10.1177/0954411914564476
John JD, Yoganandan N, Arun MWJ, Saravana KG (2018) Influence of morphological variations on cervical spine segmental responses from inertial loading. Traffic Inj Prev 19(sup1):S29-s36. https://doi.org/10.1080/15389588.2017.1403017
Phillips S, Mercer S, Bogduk N (2008) Anatomy and biomechanics of quadratus lumborum. Proc Inst Mech Eng Part H J Eng Med 222(2):151–159. https://doi.org/10.1243/09544119jeim266
Östh J, Brolin K, Carlsson S, Wismans J, Davidsson J (2012) The occupant response to autonomous braking: a modeling approach that accounts for active musculature. Traffic Inj Prev 13(3):265–277. https://doi.org/10.1080/15389588.2011.649437
Wagnac E, Aubin C, Chaumoître K, Mac-Thiong JM, Ménard AL, Petit Y et al (2017) Substantial vertebral body osteophytes protect against severe vertebral fractures in compression. PLoS One 12(10):e0186779. https://doi.org/10.1371/journal.pone.0186779
Wagnac E, Arnoux PJ, Garo A, Aubin CE (2012) Finite element analysis of the influence of loading rate on a model of the full lumbar spine under dynamic loading conditions. Med Biol Eng Compu 50(9):903–915. https://doi.org/10.1007/s11517-012-0908-6
Cook DJ, Yeager MS, Cheng BC 2015 Range of motion of the intact lumbar segment: a multivariate study of 42 lumbar spines. Int J Spine Surg 9:5. 10.14444/2005
Melnyk AD, Kingwell SP, Zhu Q, Chak JD, Cripton PA, Fisher CG et al (2013) An in vitro model of degenerative lumbar spondylolisthesis. Spine 38(14):E870–E877. https://doi.org/10.1097/BRS.0b013e3182945897
Liu R, He T, Wu X, Tan W, Yan Z, Deng Y (2024) Biomechanical response of decompression alone in lower grade lumbar degenerative spondylolisthesis–a finite element analysis. J Orthop Surg Res 19(1):209. https://doi.org/10.1186/s13018-024-04681-4
Barrey C, Jund J, Noseda O, Roussouly P (2007) Sagittal balance of the pelvis-spine complex and lumbar degenerative diseases. A comparative study about 85 cases. Eur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc 16(9):1459–1467. https://doi.org/10.1007/s00586-006-0294-6
Curylo LJ, Edwards C, DeWald RW (2002) Radiographic markers in spondyloptosis: implications for spondylolisthesis progression. Spine 27(18):2021–2025. https://doi.org/10.1097/00007632-200209150-00010
Labelle H, Roussouly P, Berthonnaud E, Dimnet J, OʼBrien M (2005) The importance of spino-pelvic balance in L5–s1 developmental spondylolisthesis: a review of pertinent radiologic measurements. Spine 30(6 Suppl):S27–S34. https://doi.org/10.1097/01.brs.0000155560.92580.90
Inoue N, Espinoza Orías AA (2011) Biomechanics of intervertebral disk degeneration. Orthop Clin North Am 42(4):487–99, vii. https://doi.org/10.1016/j.ocl.2011.07.001
Labelle H, Roussouly P, Berthonnaud E, Transfeldt E, OʼBrien M, Chopin D et al (2004) Spondylolisthesis, pelvic incidence, and spinopelvic balance: a correlation study. Spine 29(18):2049–54. https://doi.org/10.1097/01.brs.0000138279.53439.cc
Lv X, Liu Y, Zhou S, Wang Q, Gu H, Fu X et al (2016) Correlations between the feature of sagittal spinopelvic alignment and facet joint degeneration: a retrospective study. BMC Musculoskelet Disord 17(1):341. https://doi.org/10.1186/s12891-016-1193-6
Li W, Wang S, Xia Q, Passias P, Kozanek M, Wood K et al (2011) Lumbar facet joint motion in patients with degenerative disc disease at affected and adjacent levels: an in vivo biomechanical study. Spine 36(10):E629–E637. https://doi.org/10.1097/BRS.0b013e3181faaef7
Wang A, Wang T, Zang L, Yuan S, Fan N, Du P et al (2022) Quantitative radiological characteristics of the facet joints in patients with lumbar foraminal stenosis. J Pain Res 15:2363–2371. https://doi.org/10.2147/jpr.S374720
Kalichman L, Hunter DJ (2008) Diagnosis and conservative management of degenerative lumbar spondylolisthesis. Eur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc 17(3):327–335. https://doi.org/10.1007/s00586-007-0543-3
Freeman MD, Woodham MA, Woodham AW (2010) The role of the lumbar multifidus in chronic low back pain: a review. PM R J Inj Funct Rehab 2(2):142–6; quiz 1 p following 67. https://doi.org/10.1016/j.pmrj.2009.11.006
Sajko S, Stuber K (2009) Psoas major: a case report and review of its anatomy, biomechanics, and clinical implications. J Can Chiropr Assoc 53(4):311–318
Kim WD, Shin D (2023) Effects of pelvic-tilt imbalance on disability, muscle performance, and range of motion in office workers with non-specific low-back pain. Healthcare (Basel, Switzerland) 11(6):893. https://doi.org/10.3390/healthcare11060893
Adouni M, Alkhatib F, Hajji R, Faisal TR (2024) Effects of overweight and obesity on lower limb walking characteristics from joint kinematics to muscle activations. Gait Posture 113:337–344. https://doi.org/10.1016/j.gaitpost.2024.06.024
Adouni M, Aydelik H, Faisal TR, Hajji R (2024) The effect of body weight on the knee joint biomechanics based on subject-specific finite element-musculoskeletal approach. Sci Rep 14(1):13777. https://doi.org/10.1038/s41598-024-63745-x
Garay RS, Solitro GF, Lam KC, Morris RP, Albarghouthi A, Lindsey RW et al (2022) Characterization of regional variation of bone mineral density in the geriatric human cervical spine by quantitative computed tomography. PLoS One 17(7):e0271187. https://doi.org/10.1371/journal.pone.0271187
Al-Barghouthi A, Lee S, Solitro GF, Latta L, Travascio F (2020) Relationships among bone morphological parameters and mechanical properties of cadaveric human vertebral cancellous bone. JBMR Plus 4(5):e10351. https://doi.org/10.1002/jbm4.10351
Volz M, Elmasry S, Jackson AR, Travascio F (2021) Computational modeling intervertebral disc pathophysiology: a review. Front Physiol 12:750668. https://doi.org/10.3389/fphys.2021.750668
Nikkhoo M, Lu ML, Chen WC, Fu CJ, Niu CC, Lin YH et al (2021) Biomechanical investigation between rigid and semirigid posterolateral fixation during daily activities: geometrically parametric poroelastic finite element analyses. Front Bioeng Biotechnol 9:646079. https://doi.org/10.3389/fbioe.2021.646079
Sun Z, Sun Y, Mi C (2024) Comprehensive modeling of annulus fibrosus: from biphasic refined characterization to damage accumulation under viscous loading. Acta Biomater 174:228–244. https://doi.org/10.1016/j.actbio.2023.12.007
Castro APG, Alves JL (2021) Numerical implementation of an osmo-poro-visco-hyperelastic finite element solver: application to the intervertebral disc. Comput Methods Biomech Biomed Engin 24(5):538–550. https://doi.org/10.1080/10255842.2020.1839059
Barthelemy VM, van Rijsbergen MM, Wilson W, Huyghe JM, van Rietbergen B, Ito K (2016) A computational spinal motion segment model incorporating a matrix composition-based model of the intervertebral disc. J Mech Behav Biomed Mater 54:194–204. https://doi.org/10.1016/j.jmbbm.2015.09.028
Amirouche F, Solitro GF, Siemionow K, Drucker D, Upadhyay A, Patel P (2015) Role of posterior elements in the disc bulging of a degenerated cervical spine. Int J Spine Surg 9:13. https://doi.org/10.14444/2013
Kundu J, Pati F, Shim JH, Cho DW (2014) 10 - Rapid prototyping technology for bone regeneration. In: Narayan R (ed) Rapid prototyping of biomaterials. Woodhead Publishing, pp 254–284
Keaveny TM, Morgan EF, Niebur GL, Yeh OC (2001) Biomechanics of trabecular bone. Annu Rev Biomed Eng 3:307–333. https://doi.org/10.1146/annurev.bioeng.3.1.307
Singh D, Cronin DS (2017) An investigation of dimensional scaling using cervical spine motion segment finite element models. Int J Num Methods Biomed Eng 33(11):e2872. https://doi.org/10.1002/cnm.2872
Panzer MB, Fice JB, Cronin DS (2011) Cervical spine response in frontal crash. Med Eng Phys 33(9):1147–1159. https://doi.org/10.1016/j.medengphy.2011.05.004
Funding
This work is supported by the Shenzhen Science and Technology Program (Grant No. JCYJ20210324111212035), Sanming Project of Medicine in Shenzhen (Grant No. SZZYSM202311006), Natural Science Foundation of Hunan Province (Grant No. 2022JJ40696), Natural Science Foundation of Changsha City (Grant No. kq2202390), and Scientific Research Project of Traditional Chinese Medicine Bureau of Hunan Province (Grant No. B2023011).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Ziyang Liang, Xiaowei Dai, and Weisen Li are co-first authors.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liang, Z., Dai, X., Li, W. et al. Development of a spinopelvic complex finite element model for quantitative analysis of the biomechanical response of patients with degenerative spondylolisthesis. Med Biol Eng Comput 63, 575–594 (2025). https://doi.org/10.1007/s11517-024-03218-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11517-024-03218-5